The 2010-11 Budget: Prison Receivership Proposals Pose Significant Financial Risks
March 16, 2010
In February 2006, the federal court in the Plata v. Schwarzenegger case pertaining to inmate medical care appointed a Receiver to take over the direct management and operation of the state’s prison medical health care delivery system from the California Department of Corrections and Rehabilitation (CDCR). (A nonprofit corporation was subsequently created as a vehicle for operating and staffing the Receiver’s operation.) Almost two years later, the court appointed a new Receiver to continue and expand the efforts initiated by the first Receiver in bringing prison medical care up to federal constitutional standards. In this brief, we (1) provide a status report on the Receiver’s actions,
(2) present an overview of state spending on inmate medical care, (3) analyze the various requests contained in the Governor’s budget for the Receiver, and (4) identify issues and recommendations for legislative consideration.
First Receiver Restructured Inmate Medical Program. The first Receiver took a variety of actions to revamp CDCR’s medical services system. For example, he increased the range of salaries for various clinicians, and implemented salary increases for nurses, pharmacists, and other clinicians for the purpose of reducing the number of vacant positions. In addition, the Receiver revised the disciplinary process to facilitate the dismissal of incompetent physicians. He also modified the staffing classifications used to provide medical services and awarded a contract to a vendor to improve and manage pharmacy operations.
Current Receiver Implements Turnaround Plan. In June 2008, the current Receiver submitted and the federal court approved his so–called Turnaround Plan of Action for ensuring that inmates receive constitutionally adequate care. Specifically, this plan identified various deficiencies in the existing prison medical care system, as well as measurable goals to address these deficiencies. Some of these goals include reducing the number of inmate deaths, reducing the vacancies in certain clinical positions, constructing new prison health care facilities, and developing a medical information technology (IT) infrastructure. In order to implement his plan, the Receiver made significant operational changes over the past two years. For example, he established new policies related to emergency medical response, primary and chronic care delivery, and inmate medical screening and classifications.
Deaths Have Decreased... While it is difficult to assess the impact of the above changes on the quality of inmate medical care, there are some indications that conditions are improving. For example, from 2006, when the Receivership was established, to the end of 2008, the death rate in California prisons decreased from
249 per 100,000 inmates to 216. (The state’s prison death rate was slightly below the national average in 2006, according to the most recently available federal data.) In addition, the rate of “likely preventable” deaths decreased from
18 in 2006 to 5 in 2008. (Likely preventable deaths are deaths that would likely have been prevented by better medical care, as determined by a physician review.) However, the rate of “possibly preventable” deaths increased over that same time period from 48 in 2006 to 61 in 2008. (Possibly preventable deaths are deaths that may have been prevented by better medical care, as determined by a physician review.) The increase in the possibly preventable category could have been partially caused by changes made by the Receiver to make the death review process more stringent. Some deaths that would have previously been classified as non–preventable probably are now being classified as possibly preventable.
…But Significant Goals Remain Unaccomplished. Despite the reduction in death and vacancy rates discussed above, several significant goals included in the Receiver’s Turnaround Plan remain unaccomplished. These goals include the implementation of an improved health IT infrastructure, the construction of prison health care facilities, and the establishment and filling of key leadership positions (such as chief executive officers). According to the Receiver’s most recent status report to the court in January 2010, it will take several years to achieve some of these goals. He cited as barriers to progress the continued overcrowding in the prisons, the state’s fiscal crisis, and the Governor’s employee furlough program.
Figure 1 shows expenditures for inmate medical care services from 2005–06 through 2008–09 and as revised and proposed by the Governor for 2009–10 and 2010–11. As the figure shows, actual spending on such services grew from $882 million in 2005–06 (when the Receivership was established) to almost $2 billion in 2008–09, an average annual increase of 31 percent. This increase has been largely driven by greater usage of contract medical services, such as for specialty medical care provided outside prison, private ambulance transportation, and nursing and pharmacy registry usage. For example, contract medical costs have more than doubled in recent years—increasing from $394 million in 2005–06 to $845 million in 2008–09. In addition, the hiring of over 1,000 additional medical staff and the increase in salaries for physicians and nurses in recent years has also driven up inmate medical care expenditures.
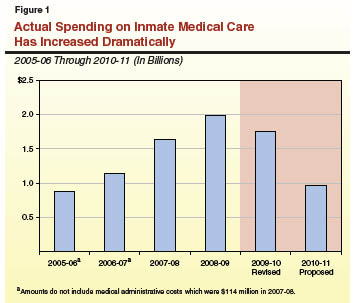
As shown in the figure, and as discussed in the next section, the revised budget for 2009–10 and the $788 million net reduction proposed by the Governor for 2010–11 differ significantly from the recent trend of significant increases in inmate medical care spending.
The Governor’s 2010–11 Budget
Proposal for the Receiver
Current Year. The Governor’s revised budget for 2009–10 reflects a total of about $1.8 billion in General Fund support for adult inmate medical operations under the control of the Receivership. As shown in Figure 1, this amount would be about $226 million less than the level of spending in 2008–09. However, the revised 2009–10 level is an increase of about $424 million, or 32 percent, from the enacted 2009–10 budget, based on the following adjustments:
- A $95 million net decrease due to various adjustments primarily related to employee compensation.
- A $407.9 million increase in base funding for contract medical expenditures, for a total of $716 million for this purpose. (For 2008–09, the Legislature approved a one–time supplemental appropriation of $487 million for contract medical expenditures.)
- A $111.3 million increase for the development and implementation of 19 IT projects (such as an electronic medical record
system) for which costs would eventually total over $800 million. (This increase would be in addition to the $45.6 million in the Receiver’s base budget for IT improvements that was provided in the 2007–08 budget.)
Budget Year. The Governor’s budget for 2010–11 proposes roughly $1 billion in General Fund support for adult inmate medical care. This is a net reduction of about $788 million from the proposed revised level of current–year spending. This net reduction would result from the following major adjustments:
- An $811 million (or roughly 50 percent) unallocated reduction in 2010–11, which would be in addition to a $181 million unallocated reduction contained in the 2009–10 budget. As part of the special session on the budget, the Legislature approved the new $811 million reduction in legislation. However, the Governor vetoed the legislation because he felt that the package of special session legislation passed by the Legislature did not go far enough in addressing the state’s current General Fund shortfall.
- A $199 million decrease to reflect a reduction in projected contract medical expenditures.
- A $132.5 million increase to continue the development and implementation of the 19 IT projects referenced above.
- A $33.6 million increase for 346.7 additional nursing positions proposed to reduce the reliance on registry nurses in meeting existing workload needs and to distribute medication to inmates in a more timely and efficient manner.
In addition, the budget includes $45.8 million to extend for one additional year a temporary augmentation that was provided in each of the prior three fiscal years for pharmaceuticals and medical supplies. (Although the Receiver is also in the process of proposing a health care construction program, none of the proposed projects are reflected in the Governor’s budget for 2010–11 and, thus, are not the focus of this analysis.)
Based on our review of the Governor’s budget proposals related to inmate medical care, we have identified several issues that merit legislative consideration.
Significant Risk in Achieving Proposed Unallocated Reduction. The Governor’s proposed $811 million unallocated reduction assumes that per inmate medical costs can be reduced from $11,627 per year to $5,740 per year. The administration indicates that such a reduction would bring the state’s per inmate medical costs roughly to the amount that New York spends on such medical care. According to the administration, this reduction could be achieved through a variety of unspecified measures, such as reducing staff to patient ratios, increasing the utilization of telemedicine, and reducing clinical salaries.
In order to achieve savings of this magnitude, the Receiver would need to implement major operational changes by July 1, 2010. However, at the time of this analysis, the administration had not presented a specific plan as to how the Receiver would achieve any of the proposed savings. (It is important to note that the Receiver has been unable to identify how a much smaller unallocated reduction of $181 million in the 2009–10 budget will be achieved.) Given the absence of such a plan and the amount of lead time required to implement the major operational changes that would need to occur by July 1, 2010, we believe that assuming the level of savings contained in the Governor’s 2010–11 budget proposal poses significant risks.
Pending Plan to Achieve Reduction Could Affect Staffing Requests. In developing a plan for achieving the proposed $811 million unallocated reduction, the administration informs us that they are examining all options to reduce inmate medical care costs, including proposals that would effectively reduce the population of inmates with medical needs. For example, one proposal could include releasing certain elderly and infirm inmates early from prison and placing them on parole based on their medical status. Our analysis indicates that such population reduction proposals could reduce the need for the additional nursing positions requested in the Governor’s budget.
We also note that these particular staffing requests do not take into account the impact on the size of the inmate population of the various policy actions that were adopted as part of the 2009–10 budget (such as no longer returning to prison certain parole violators with no record of serious, violent, or sex offenses). The staffing requests also do not take into consideration the Governor’s 2010–11 budget proposal to require that certain felony offenders serve a maximum sentence of one year and one day in county jail in lieu of a state prison sentence. Thus, it is unclear at this point whether these additional nurses would be needed after the 2009–10 budget actions and those additional population reductions proposed in the 2010–11 budget were taken into account.
Receiver’s IT Plan Raises Significant Project Risks. Our analysis indicates the 19 IT projects proposed by the Receiver generally address deficiencies identified by the Plata court and that are to be remedied in the Turnaround Plan. In addition, a few of the projects (such as telemedicine and the utilization management system) could potentially reduce future inmate medical care costs. However, we find that the Receiver’s IT plan is overly ambitious in terms of its scope and is very costly. For example, the number and size of the IT projects proposed by the Receiver greatly exceed the number of projects that are normally managed by most state agencies at any one point in time.
As we have indicated over the years, limiting the size of an agency’s portfolio of IT projects can help reduce the heightened level of risks and management challenges that typically arise when an agency undertakes multiple projects simultaneously. Moreover, many of the 19 projects proposed by the Receiver are interdependent on one another, increasing the risk of (1) a cascade of missed deadlines and substantial delays in the completion of projects and (2) significant cost overruns if any of the projects was not completed on schedule.
Receiver Unable to Account for Ongoing Funding for IT Projects. As previously mentioned, the state budget for each of the past three fiscal years has provided the Receiver $45.6 million (for a total of about $137 million) to support IT improvements. However, at the time of this analysis, the Receiver’s office was unable to provide sufficient information in response to our questions on how these funds have been spent. For example, the office has not provided a detailed accounting on how much of the funds was spent on each of the 19 IT projects. Moreover, based upon the information given to us in support of these requests, the Receiver’s office does not appear to account for this $45.6 million in available funding in its 2010–11 IT budget request.
Although the Receiver and the federal courts continue to independently and actively exercise their authority over CDCR’s medical services programs, the Legislature continues to bear the responsibility under the State Constitution to appropriate funds and enact an annual budget to support CDCR. As we discussed in our Analysis of the 2007–08 Budget Bill, we believe it is possible and desirable for the Legislature and the Receiver to exercise their respective responsibilities under a cooperative approach that will strengthen fiscal controls over medical services as well as improve the quality of care provided to inmates.
Thus, to the extent that it is practical, the Legislature should apply its standard budgetary processes to carefully review and act upon each 2010–11 budget proposal submitted by the administration on behalf of the Receiver. Specifically, if the Legislature believes that a particular proposal is overbudgeted or overstaffed on a workload or other technical basis, we believe that it should act to modify the proposed expenditures. Accordingly, we recommend the Legislature take the following budgetary actions.
Require Detailed Plan to Achieve Savings. We recommend that the Legislature require the administration to present at budget hearings a detailed plan on how the proposed $811 million in savings will be achieved. This plan should include (1) the specific proposals that the Receiver would implement, (2) a timeline of when each proposal would be implemented, (3) the estimated savings that would result from each proposal, (4) any statutory changes (or federal court actions to waive state legal requirements) that would be required in order to implement the plan, and (5) an assessment on how previously adopted and pending proposals to reduce the size of the inmate population would affect the need for the additional nursing positions proposed in the Governor’s budget.
Withhold Action on Staffing Requests. Pending the submission and our review of the above plan, we withhold recommendation on the Governor’s requests for additional nursing positions totaling $33.6 million.
Prioritize the Most Critical IT Projects. While we recognize the desire of the Receiver to develop and implement the 19 IT projects as early as possible, given the state’s current General Fund shortfall, the state cannot afford to make a multiyear commitment of $800 million to so many projects at once. Moreover, as discussed above, we believe that the Receiver’s IT plan is overly ambitious and poses significant risks. Thus, we suggest that the Legislature fund only the most critical IT projects in the budget year and delay funding for the less critical projects.
Specifically, we recommend providing funding for only those projects that (1) will provide the basic infrastructure needed for some of the other projects (such as the healthcare network, data center, and the clinical data repository) and (2) could result in significant operational savings (such as telemedicine and utilization management). We estimate that this would reduce the Governor’s budget request by about $42 million (from $111.3 million to $69 million) in 2009–10 and by about $153 million (from $243.8 million to $91 million) in 2010–11. (Our estimate for the budget year recognizes that the $45.6 million in the Receiver’s base budget for IT is available to help support the costs of the projects.) The additional resources needed to support our recommended projects over the next five years would be roughly $300 million.
Our proposal for the Receiver to focus on the most critical projects would also allow his office to demonstrate that it can effectively manage a smaller number of projects before undertaking a comprehensive IT overhaul. We recognize that the Receiver may believe that a different mix of projects should be funded in the budget year than those we recommend above. Thus, the Legislature may want to ask the Receiver to report at budget hearings on which of the 19 projects he believes are of the highest priority.
Return to LAO 2010-11 Budget: Judicial and Criminal Justice Table of Contents
Return to LAO 2010-11 Budget: Full Table of Contents
Return to LAO Home Page