Legislative Analyst's OfficeAnalysis of the 2001-02 Budget Bill |
The California Department of Corrections (CDC) is responsible for the incarceration, training, education, and care of adult felons and nonfelon narcotic addicts. It also supervises and treats parolees released to the community.
The department now operates 33 institutions, including a central medical facility, a treatment center for narcotic addicts under civil commitment, and a substance abuse treatment facility for incarcerated felons. The CDC system also includes 12 reception centers to process newly committed prisoners; 16 community correctional facilities; 38 fire and conservation camps; the Richard A. McGee Correctional Training Center; 34 community reentry, restitution, and drug treatment programs; 136 parole offices; and 4 outpatient psychiatric services clinics.
The budget proposes total expenditures of $4.8 billion for CDC in 2001-02. This is $220 million, or 5 percent, above the revised estimate for current-year expenditures. The primary causes of this increase are the growth in the inmate population, increases in staff compensation, equipment replacement, and increased costs for medical services.
Under the budget plan, the CDC workforce would grow by about 434 personnel-years, or about 1 percent, above the projected 2000-01 staffing level. This projected growth is significantly less than the anticipated current-year growth in the CDC workforce, estimated to be about 4,000 personnel-years, or 9.5 percent.
Expenditure Growth Continues to Slow. The 2001-02 budget proposal represents a slower overall rate of growth in CDC expenditures. During the past ten years, the average annual growth rate has been about 8 percent. If the budget were adopted as proposed, the proposed 5 percent increase in CDC expenditures would be the smallest since 1978-79, except for 1992-93—a year when the state faced an unusually large revenue shortfall and CDC spending actually decreased slightly. As discussed below, the proposed slowdown in correctional spending growth is associated with a slowdown in the growth in the inmate population and related growth in CDC staffing.
However, despite overall expenditure growth trends in CDC, the average cost of providing supervision for each inmate is increasing significantly. After holding stable for many years, the average cost of maintaining an offender in the CDC prison system (excluding capital outlay costs) would grow to $25,607 in the budget year, an increase of about 13 percent over 1999-00. The average cost of supervising a parolee remains stable at $2,636 per offender under active supervision.
General Fund Expenditures. Proposed General Fund expenditures for the budget year total almost $4.7 billion, an increase of about $260 million, or 6 percent, above the revised estimate for current-year General Fund expenditures.
The General Fund contribution to the proposed budget would grow more than the CDC budget overall. One major reason is a decline in the availability of bond funds to partly offset CDC costs. In prior years, bond funds that were no longer needed for completed prison construction projects were used to offset the ongoing payments on lease-payment bonds. For 2001-02, these offsetting payments are budgeted at about $13 million, a decline of about $28 million, or 69 percent, below the current year. Because the state has nearly exhausted these surplus bond funds, larger General Fund appropriations to CDC are now required to pay off these lease-payment bonds.
Federal Fund Expenditures. The Governor's budget assumes that the state will receive about $189 million from the federal government during 2001-02 as partial reimbursement of CDC's cost (estimated to be $551 million in the budget year) of incarcerating inmates in prison and supervising felons on parole who are illegally in the United States and have committed crimes in California. This is a slightly higher level of funding than the state is estimated to receive in the current year. The federal funds are not included in CDC's budget display, but instead are scheduled as "offsets" to its total state General Fund expenditures.
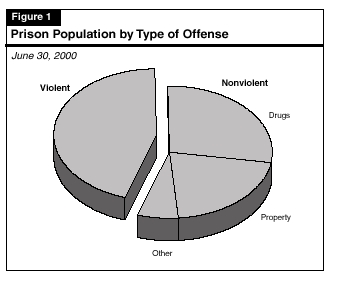
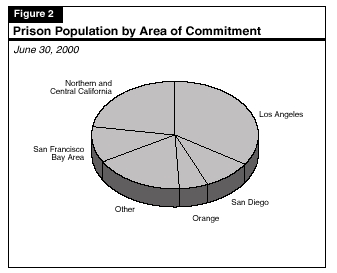
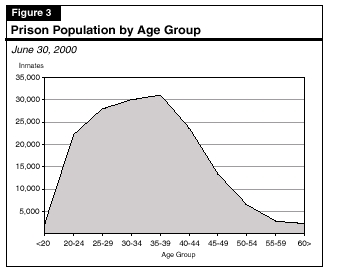
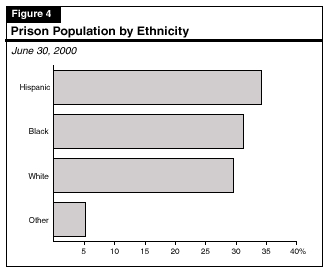
Figures 1 through 5 illustrate the characteristics of the state's prison population, which was 162,000 as of June 30, 2000. About 93 percent of the population is male. The charts show:

The California Department of Corrections (CDC) is projecting slower growth in the prison population than the state experienced through much of the 1990s. The CDC projections suggest that the number of inmates will exceed 185,000 by June 2006. Recent prison population data suggest, however, that the growth rate is even slower than assumed in the Governor's budget and that the population is continuing to stabilize.
Inmate Population Growth. As of June 30, 2000, the CDC housed 162,000 inmates in prisons, fire and conservation camps, and community correctional facilities. Based on the fall 2000 population forecast prepared by the CDC, the inmate count would reach about 163,898 by June 30, 2001, and increase further to 166,876 by June 30, 2002. These figures represent an annual population increase of 1.2 percent in the current year and 1.8 percent in the budget year. As can be seen in Figure 6, this projected trend, if it actually occurs, would be significantly slower than the 10 percent average annual inmate population growth the state experienced during the past decade.

The CDC projections assume that the population will increase over the following four years, reaching 185,865 inmates by June 30, 2006. This represents an average annual population increase of about 3 percent over the six-year period from 1999-00 through 2005-06.
Parole Population Growth. As of June 30, 2000, the CDC supervised 119,298 persons on parole. The fall 2000 projections assume that the parole population will be 122,880 as of June 30, 2001, and will increase slightly to 125,164 by June 30, 2002. These figures assume a parole population increase of 3 percent in the current year and an increase of 2 percent during the budget year.
The fall 2000 projections also assume that the population will remain fairly stable during the following four years, reaching a total of 128,391 parolees by June 30, 2006.
Change From Prior Projections. The fall 2000 projection of the inmate population has increased from the prior CDC forecast (spring 2000), which was the basis for the 2000-01 Budget Act. The new fall 2000 forecast for June 30, 2001 is about 3800 inmates higher than the spring forecast. As can been seen in Figure 7, the differences between the spring 2000 and fall 2000 inmate projections generally widen with time over the projection period. By 2004-05, the difference is almost 7,500 inmates, or the equivalent of about two prisons filled to overcrowding levels.
|
Figure 7 |
|||
|
Total Inmate Population |
|||
|
|
Projection as of: |
||
| June 30 Population a |
Spring 2000 |
Fall 2000 |
Difference |
|
2001 |
160,060 |
163,898 |
3,838 |
|
2003 |
163,248 |
170,160 |
6,912 |
|
2005 |
173,000 |
180,445 |
7,445 |
|
a For selected years. |
|||
As regards the parole population, the fall 2000 projection also reflects a significant increase relative to the prior spring 2000 CDC forecast. The new fall 2000 forecast for June 30, 2001 is 2,581 parolees more than the spring forecast. As can be seen in Figure 8 , the differences between the spring 2000 and fall 2000 parole projections also widen with time over the projection period until the differential exceeds 14,700 parolees at the end of 2004-05.
|
Figure 8 |
|||
|
Total Parole Population |
|||
|
|
Projection as of: |
||
| June 30 Population a |
Spring 2000 |
Fall 2000 |
Difference |
|
2001 |
120,299 |
122,880 |
2,581 |
|
2003 |
115,559 |
126,934 |
11,375 |
|
2005 |
113,892 |
128,631 |
14,739 |
a For selected years. |
|||
Why the Forecasts Changed Between Spring and Fall 2000. According to CDC, the higher projections in the inmate and parole populations are based on an increase in the rate of parole violators returned to custody and an increase in felon new admissions.
Potential Risks to Accuracy of Projections. As we have indicated in past years, the accuracy of the department's latest projections remain dependent upon a number of significant factors. These include:
Significant changes in any of these areas could easily result in a prison growth rate higher or lower than the one contained in CDC's projections. Given the slowdown in prison inmate growth that has already occurred in the last two years, it is possible now that, at least in the short term, the prison population may be stabilizing.
Actual Inmate Count Is Lower Than Fall Projections. During the first half of 2000-01, the prison population had been projected to increase slightly by 153 inmates over the prior year. Instead, it decreased by about 1,300 as shown in Figure 9. Given the historical pattern of inmate population growth, it is likely that this downward trend will reverse itself in the spring of 2001, when more inmates normally are admitted into the prison system than at other times of the year. Even if there is a turnaround in the trend this spring, however, it appears unlikely that CDC will experience a population gain in the current year of 1,898 inmates as forecast in the fall 2000 projections. Actual growth may be less than 1,000 inmates.

Several factors appear to have caused the inmate population to drop during the latter part of 2000 instead of growing as had been projected. The CDC data indicate that fewer parole violators than projected are being returned to prison by administrative actions of the Board of Prison Terms (BPT), and that they are serving slightly less time in prison than had been expected. Moreover, fewer parolees than anticipated are being returned to state prison by the courts.
A number of factors have probably contributed to this result, including many of the same ones—the improved economy and dropping crime rates—that are behind the drop in felon admissions generally. But it appears probable that one factor keeping more parolees out of prison is the expansion of services for parolees that began in 1998-99, such as drug treatment, casework services, and job placement, to assist these offenders in making their transition back to the community.
The CDC data indicate that the parole "failure rate"—the rate at which parolees come back to prison by actions of BPT and the courts—was equal to about 66 percent of the parole population during the second half of 2000. While that failure rate is high compared to other states, the data suggests that there has been little change in California's parole failure rate since 1999.
Budget Modified to Reflect Trend. The Governor's January budget proposal for CDC is ordinarily based upon CDC projections released the previous fall. However, that is not the case for the proposed 2001-02 CDC spending plan. In preparing the budget, the Department of Finance (DOF) made fiscal adjustments to account for differences between the fall 2000 projections and actual inmate and parole population counts.
Specifically, DOF reduced caseload funding for the state prisons by the equivalent of 606 inmates for 2000-01 and by 1,501 inmates for 2001-02. The department increased caseload funding for parolee supervision by the equivalent of 80 more parolees for 2000-01 and 454 parolees for 2001-02.
Because of these inmate and parole population adjustments, DOF has estimated that about $7 million less would be needed to handle the prison and parole caseload during 2000-01. Similarly, DOF adjustments mean that about $16 million less in funding would be provided to handle the prison and parole caseload during 2001-02 than if the budget plan were based on CDC's population figures.
We recommend that the 2001-02 budget request for inmate and parole population growth be reduced by $61 million. This reduction reflects a continuing decrease in the inmate population, as well as the impact of Proposition 36, the drug diversion initiative recently approved by the voters, on the prison inmate and parolee population. In regard to the current year, we estimate that California Department of Corrections (CDC) caseload expenditures will be $7 million less than budgeted. Further changes to the CDC budget for the current and budget years should be considered following review of the May Revision. (Reduce Item 5240-001-0001 by $61 million.)
As indicated earlier, CDC's fall 2000 population projections appear to have overestimated the number of inmates who are being incarcerated. The Governor's budget, as submitted, adjusts CDC's fall 2000 projections to reflect a slower growth rate. However, based on our review of more recent data not available when the budget plan was drafted, we estimate that if current trends hold, the downward adjustments made by the Governor's budget will be insufficient.
In addition, Proposition 36, the Substance Abuse and Crime Prevention Act, which was passed by voters on November 7, 2000, is expected to further slow growth in the prison population. Proposition 36 requires that persons convicted of nonviolent drug possession offenses be placed on probation and receive drug treatment, rather than be incarcerated in state prison. Similarly, the measure will redirect parole violators who commit nonviolent drug possession offenses into treatment rather than returning them to prison. Although Proposition 36 will go into effect on July 1, 2001, the CDC fall 2000 projections do not take into account the significant decreases in the inmate and parolee populations that will occur as a result of this measure. Furthermore, the DOF has not made fiscal adjustments to reflect the impact of Proposition 36 on caseload funding in the budget year.
Our estimates of the CDC inmate population, which take into account more recent inmate population trends as well as the impact of Proposition 36, are shown in Figure 10.
|
Figure 10 |
||
|
Inmate Population Assumptions a |
||
|
2000-01 |
2001-02 |
|
|
California Department of Corrections |
162,684 |
164,826 |
|
Governor's Budget |
162,078 |
163,325 |
|
Legislative Analyst's Office |
161,548 |
158,503 |
a Average daily population. |
||
Current-Year Effect. Based on the inmate population as of the end of December 2000, we estimate that the average daily population of the prison system in 2000-01 will be about 530 inmates below the caseload actually funded in the Governor's budget plan. We further estimate that the average daily parole population will be about 480 inmates lower than the caseload funded in the Governor's budget plan. The net effect of these two changes would be a savings in the current year of $7 million.
Budget-Year Effect. We anticipate that this caseload trend will carry over into 2001-02. Based on available population counts and our projections of the impact of Proposition 36 on the CDC inmate population, we estimate that the average daily prison population in the budget year will be about 4,800 fewer inmates than the number assumed in the proposed budget. We further estimate that the average daily parole population will be about 3,100 lower than assumed in the budget plan. (These estimates include a 3,800 decrease in the inmate population and a 1,050 decrease in the parolee population due to the impact of Proposition 36.) Based on these calculations, we believe that the CDC budget for handling its inmate and parole caseloads is over budgeted by $61 million.
The CDC will issue updated population projections in spring 2001 that form the basis of the department's May Revision proposal. The spring 2001 projections will take into account the effect of Proposition 36 on the inmate and parolee population. At that time, we will review whether further adjustments to CDC's funding for inmate and parole caseloads are warranted.
Analyst's Recommendation. In summary, we recommend that the 2001-02 CDC budget be reduced by $61 million from the General Fund primarily due to the combined effect of slower growth in the underlying CDC inmate population and the decrease in the inmate and parolee populations due to Proposition 36. The current-year budget is also likely to reflect savings of about $7 million due to slower CDC caseload growth. We recommend that the Legislature consider making further CDC caseload adjustments at the time of the May Revision.
We withhold recommendation on the California Department of Corrections' (CDC) plan for housing the projected increase in the prison population because the underlying rate of growth in the inmate population is slowing and the caseload decrease resulting from implementation of Proposition 36 have made elements of the plan obsolete. We anticipate the CDC will revise the housing plan at the time of the May Revision.
Prison Overcrowding to Continue. The Governor's housing plan provides for the continuing overcrowding of day rooms, gyms, and housing units at various existing prisons. However, many existing prison bed activation proposals included in the plan are unlikely to occur because of the slowing in the rate of prison population growth and the decrease in the inmate population as a result of Proposition 36.
The housing plan assumes the state will complete construction and activate 1,000 administrative segregation beds for high-risk inmates on the grounds of the existing state prisons, as authorized by the Legislature in 1998. The Governor's budget does not propose to construct any new state-operated prisons.
Analyst's Recommendation. Because the inmate population is running below the fall 2000 projections upon which the CDC housing plan was based and because the projections do not reflect the impact of Proposition 36 on the inmate population, it is likely that the plan will change significantly by the May Revision. Thus, we withhold recommendation on the plan at this time pending receipt of CDC's revised prison inmate population projections and the updated housing plan provided in the May Revision.
In 1996, two inmates with developmental disabilities filed a lawsuit against the California Department of Corrections (CDC) which stated that the department discriminated against them due to their disability. Prior to trial in 1998, CDC and the plaintiffs negotiated the development of a remedial plan to screen for and provide appropriate services to developmentally disabled inmates.
While the CDC remedial plan increases services to inmates, the plan does not address the issue of services for developmentally disabled parolees in the community. We recommend the Legislature direct CDC, in consultation with other state agencies, to evaluate the assessment process and need for services of developmentally disabled parolees and develop a plan for providing those services.
In this section, we review the CDC plan for providing services to developmentally disabled inmates and parolees. We begin by describing the interaction between developmentally disabled offenders and the criminal justice system and how these individuals eventually become CDC inmates. Next, we discuss the implementation status of the CDC plan to screen inmates for developmental disabilities and provide appropriate services for identified inmates. We follow this with our concerns about the current remedial plan and recommendations to the Legislature based on our findings.
State law (Section 4521 of the Welfare and Institutions Code) defines a developmental disability for the purpose of determining eligibility for developmental services in the community. Such a disability is defined as a mental or neurological impairment that originates before a person's eighteenth birthday, constitutes a substantial disability, and continues indefinitely. These disabilities include mental retardation, cerebral palsy, epilepsy, autism, and related conditions.
Approximately 155,000 Californians annually receive services in the state's publicly funded developmental disability service system. The state Department of Developmental Services (DDS) contracts with 21 nonprofit regional centers to coordinate educational, vocational, and residential services for this population. In addition, for individuals needing 24-hour care and supervision, DDS operates about 4,000 beds in five state developmental centers.
Developmentally Disabled Offenders in the Criminal Justice System. Some research indicates that as many as 22,000, or 4 percent, of individuals in California jails and prisons have a developmental disability, the severity of which can vary greatly. Developmentally disabled offenders often do not become eligible for probation due to their limited skills and lack of employment and education prospects. They are also ineligible for diversion programs, when available, due to their condition.
No Specialized Services for Developmentally Disabled Inmates. Prior to 1999, inmates with developmental disabilities received no special services and were treated as part of the general prison population. Research indicates these inmates were more likely to be abused or victimized by other inmates and, due to a tendency to react physically to these situations, were also more likely to get into fights. This poor institutional behavior resulted in many inmates taking up additional staff resources and being moved to higher and more costly security levels. The limited ability of these inmates to earn credits, through education or work programs, toward the reduction of their sentence made it difficult for them to become eligible for parole as quickly as other inmates.
Clark v. State of California. On April 22, 1996, two inmates with developmental disabilities who were incarcerated within CDC filed a class action suit against the State of California, the Governor, CDC, and various prison officials alleging that they had been discriminated against on the basis of their disability in violation of the Equal Protection Clause, the Americans with Disabilities Act, and the Rehabilitation Act. The inmates claimed that they did not receive adequate accommodations, protection, and services necessary for adaptation to a prison. Prior to the trial in 1998, the parties engaged in negotiations, which resulted in a settlement agreement outlining the terms under which the state would comply with the law by providing access to its programs and services for inmates and parolees with developmental disabilities.
Summary of the Settlement. The remedial plan resulting from the settlement agreement, known as the Clark plan, indicated that CDC would establish a Developmental Disability Program (DDP). Under this program, CDC would screen all inmates for developmental disabilities and place identified inmates in designated institutions with the staffing and program capabilities to meet their needs. Figure 11 summarizes the key features of the agreement, many of which are discussed in more detail below.
|
Figure 11 |
|
Key Features of the CDC Developmental |
|
|
|
|
|
|
|
|
|
|
In the 1999-00 Budget Act, the Legislature appropriated $1.8 million to CDC to begin implementing the remedial plan to provide services to developmentally disabled inmates at ten institutions. The CDC estimated that approximately 2 percent of inmates would be found to be developmentally disabled at reception and that the funding provided would be sufficient to screen all inmates and provide appropriate services. It is expected that these costs will continue and could increase in the long term.
Screening Procedure. Under the Clark remedial plan, all inmates must be screened at reception for developmental disabilities using a standardized screening process. In addition, CDC must screen all existing inmates for developmental disabilities.
The CDC developed a screening tool to assess an inmate's cognitive abilities and functioning skills. It appears, however, that this tool differs substantially from that used in the state developmental services system in two respects. First, the CDC process may identify an individual as having a development disability, even when it is difficult to clearly state that the disability occurred prior to age 18. Such persons may not qualify as developmentally disabled under the regional center definition. In addition, the CDC screening process captures inmates who experience mental retardation as a result of substance abuse. Because it typically takes years for the mentally disabling effects of substance abuse to be felt, these individuals often may not qualify under the regional center definition because their disability is thought to have occurred after age 18.
The second way in which CDC screening appears to differ from that used by regional centers is the extent to which a disability impacts an individual's ability to function without assistance. The Welfare and Institutions Code definition requires there to be a substantial disability. The CDC, on the other hand, appears to include ability to function adequately in a correctional environment in its definition of developmental disability. Therefore, someone with mild retardation who is classified as developmentally disabled for the purposes of receiving services in CDC may not be eligible for regional center services. Overall, CDC appears to use a broader definition of what constitutes developmental disability than DDS.
The situation that results from the use of two differing sets of screening standards is that inmates identified by CDC as being developmentally disabled and needing services within a prison may not meet the regional center eligibility requirements as provided for in existing law.
Since December 1999, CDC has been screening all new admissions and parole violators processed through the reception centers. Currently, CDC is not screening inmates in the existing population for developmental disabilities, although the department intends to begin by June 2001 and will complete all screenings by mid-2002. To date, about 1,500 or 1 percent of inmates processed through reception centers have been found to have a developmental disability, as defined by CDC, of which 85 percent have been found to have mild retardation.
Housing and Staffing. After determining the extent of the developmental disability, these inmates are assigned to 1 of 13 designated DDP institutions where they are housed apart from the general population. Inmates with mild retardation are housed together and inmates with moderate disabilities or at risk for victimization are housed together. If developmentally disabled inmates have additional health or psychiatric problems, they are housed at DDP facilities which are designed to address these concerns.
All DDP institutions have additional staff to provide specific services to developmentally disabled inmates. Clinical staff is augmented with correctional officers, counselors, and teachers trained to work with developmentally disabled inmates.
Staff Training. Under the remedial plan, CDC must provide training to all staff who screen, interact, and have responsibility for inmates and parolees designated as developmentally disabled. Currently, all required CDC staff have completed the training mandated under the plan. The training, which is provided in a self-study or two-hour classroom format, provides basic information on developmental disabilities including:
Education. At designated DDP institutions, CDC provides instructors with special education credentials who will develop individual education plans for developmentally disabled inmates. Disabled inmates will also be eligible for vocational education programs, as long as they meet the same requirements as other inmates and are able to perform essential functions of the assignment.
Parole Services. The CDC plans to make reasonable accommodations to ensure that developmentally disabled parolees understand the terms of parole, are aware of available services in the community, and have access to attorney representation in parole revocation hearings. However, specific actions to achieve these objectives are not detailed in the remedial plan.
The CDC has taken significant steps to improve screening and treatment services for inmates whom it has identified as developmentally disabled. While these programs and services have been beneficial to inmates in prison, parolees with similar disabilities generally do not receive specialized services. In addition, CDC has not collaborated with other state agencies which serve developmentally disabled parolees, such as DDS and BPT, to develop a continuum of services for this population which extends into their parole period in the community.
Lack of Comprehensive Plan for Parole Services. As stated previously, the remedial plan developed under the Clark settlement includes some minor provisions for parole services. The services provided under the plan, however, do not differ very much from services already being provided to all parolees. The CDC indicates it eventually plans to provide targeted services for developmentally disabled parolees, including creating smaller specialized caseloads. A well-developed comprehensive plan, specifying program services and coordination with local service providers, does not yet exist, however.
Lack of CDC Coordination With Other State Agencies. Although DDS is the primary state agency charged with providing services to the developmentally disabled, both in the community and in developmental centers, CDC has not coordinated with DDS on the development of its remedial plan or on a plan to provide specialized services to developmentally disabled parolees in the community. Currently, levels of coordination between parole agents and regional center staff vary widely by region due to a lack of a structured relationship. Inmates are advised, upon parole, of services available to them through regional centers. However, regional center staff do not assess inmates prior to release and do not provide any input in developing a parolee's discharge plan.
The BPT, which considers parole release for all persons sentenced to state prison under the indeterminate sentencing laws and is responsible for suspending and revoking parole status, was not named as a defendant in the Clark case. Due to its role in determining if developmentally disabled offenders remain on parole, BPT should be included in the development of a parole services plan which ensures that these offenders receive accommodations for their disabilities in parole hearings. Currently, however, developmentally disabled inmates are generally treated the same as higher functioning inmates and receive no additional services.
Limited Parolee Eligibility for Regional Center Services. As stated previously, regional centers use standards and screening techniques which differ from those used by CDC in identifying inmates and parolees with developmental disabilities. As a result, individuals identified in the CDC screening process may not be eligible for regional center services when paroled into the community.
We recommend the Legislature adopt supplemental report language directing the California Department of Corrections (CDC), in consultation with Department of Developmental Services, the State Council on Developmental Disabilities, and the Board of Prison Terms, to undertake a study of issues relating to parolees with developmental disabilities. This study would focus on problems relating to eligibility and screening and would require CDC to develop a plan for meeting the service needs of parolees with developmental disabilities.
Developing a Collaborative Parole Services Plan. The CDC has taken steps to provide appropriate services to inmates with developmental disabilities. The department, however, has not developed a comprehensive plan for providing services to inmates once they are released on parole. Given the high level of recidivism among this population, a plan which provides developmentally disabled parolees with appropriate services and monitoring in the community could improve public safety by assisting these offenders in reintegrating into the community. Such a plan should focus on lower specialized parole agent caseloads to allow for increased supervision, and steps for increasing coordination among CDC and other agencies, such as BPT and DDS. This would also would help ensure that developmentally disabled parolees receive necessary accommodations for their disabilities, such as assistance in accessing community services.
Increasing Parolee Access to Regional Center Services. Prior to CDC undertaking such a collaborative effort, the state needs to better understand the problems of providing case management and related services to two groups of parolees with developmental disabilities. The first group consists of those who clearly meet the regional center standard of eligibility. The second group consists of those individuals who have a mental impairment, including mild retardation, but who do not meet the regional center definition, either because their disability is not "substantial," or because the date of onset was after age 18 or is indeterminable because of the cumulative effects of substance abuse.
A number of service options exist, each with its own set of issues. One option is for regional centers to better incorporate those eligible for its services into its caseload. A second option is for regional centers to expand its services to include that segment which currently does not meet its eligibility criteria. This alternative, however, raises serious cost and equity questions relating to lack of available services to individuals with similar levels of disabilities who are not parolees. A third option is for CDC, in consultation with DDS, to contract directly with community providers to deliver services to parolees identified by CDC as having a developmental disability but who are ineligible for regional center services. Prior to selecting an option more information is needed about the target population.
Analyst's Recommendation. We recommend the Legislature direct CDC, in consultation with other appropriate state agencies such as DDS, the State Council on Developmental Disabilities and BPT, to undertake a study of the size, nature, and service needs of parolees with developmental disabilities. This study should include:
Accordingly, we recommend the adoption of the following supplemental report language:
It is the intent of the Legislature that the California Department of Corrections (CDC), in consultation with the Department of Developmental Services, the State Council on Developmental Disabilities, and the Board of Prison Terms, conduct a study of the size, nature, and service needs of parolees with developmental disabilities. The study shall include, but not be limited to, the following matters: a review of the assessment criteria used by both CDC and regional centers to identify developmental disabilities and an identification of differences and inconsistencies between the two systems, a determination of the number of parolees who meet the CDC definition and the extent to which they do or do not meet the regional center definition, an examination of the extent to which regional centers currently incorporate eligible parolees with developmental disabilities into their service system, and a plan to address identified service needs and reduce the recidivism rates of developmentally disabled parolees. The findings of this study shall be reported to the Legislature by March 1, 2002.
We recommend approval of the proposal to expand substance abuse treatment services to additional inmates and parolees. We also recommend a reduction of $112,000 proposed for custodial staff overtime salaries in order to attend substance abuse training, because it duplicates compensation already being paid to correctional officers for overtime spent in training. We further recommend the adoption of supplemental report language directing the department to report on its progress in activating proposed substance abuse treatment slots. (Reduce Item 5240-001-0001 by $112,000.)
The budget proposes $3.9 million from the General Fund and nine positions to add 500 substance abuse treatment slots for inmates and parolees. The proposed increase would support contracted in-custody treatment services, community-based services, drug testing, overtime costs for staff training, and general operating expenses. The new program slots will serve male felons and civil addicts at the California Rehabilitation Center (CRC) and at the Adelanto Community Correctional Facility.
Implementation of the proposal would result in ongoing costs of $6.6 million in 2002-03 and beyond. This ongoing cost primarily reflects (1) full-year operation costs and (2) the additional community services for inmates who have completed the in-prison portion of the treatment.
Background. The CDC's Office of Substance Abuse Programs currently administers treatment and recovery programs, which include 15 in-prison treatment programs serving 6,650 inmates annually and parolee service networks serving about 4,000 parolees annually. Contractors provide alcohol and drug abuse treatment that emphasizes changing inmate behaviors as opposed to treating only the substance addiction.
Currently, CDC in-prison treatment programs are operating at about 93 percent of capacity. The department anticipates that an additional 1,500 slots at various institutions will be activated by the end of the current year.
Increase in Substance Abuse Slots Is Justified. Although the implementation of Proposition 36 will reduce the number of new admissions and parole violators, there will continue to be a need for substance abuse treatment services for the current inmate population. Currently, there is a waiting list of 260 inmates for treatment at CRC and no treatment slots available at the Adelanto facility. Providing funds to address an existing waiting list at CRC and the lack of treatment services at the Adelanto facility is consistent with the department's objective to increase treatment availability and justifies further investment.
Overtime Salaries for Training Duplicates Existing Compensation. The proposal includes $112,000 to fund overtime salaries for custodial staff to attend training in substance abuse issues. This funding duplicates existing funding since each custody officer already receives annual compensation for 52 hours of on-site training under the 7k program (a reference to Section 207 [k] of the federal Fair Labor Standards Act.). Since the proposed training could qualify for compensation under the 7k program, the additional overtime funding is not needed.
Analyst's Recommendation. For the above reasons, we recommend approval of the proposal to expand substance abuse treatment slots. However, we recommend a reduction of $112,000 for overtime spent in training because custody officers are already compensated for 52 hours of training under the 7k program.
Due to the passage of Proposition 36, there could be a reduction in the number of inmates in need of in-prison drug treatment services and an increase in the number of parolees in need of treatment or aftercare services. The Legislature should increase oversight of CDC substance abuse programs including additional treatment slots to ensure treatment resources are being allocated effectively between in-prison treatment services and parole treatment services. We, therefore, recommend the adoption of supplemental report language requiring the department to report on its progress in implementing substance abuse treatment slots. The following language is consistent with this recommendation:
The California Department of Corrections (CDC) shall report to the Legislature by January 1, 2002, on its progress in implementing substance abuse treatment slots. The report should identify the number of occupied treatment slots at each facility, the number of inmates waiting for treatment, the number of parolees in each type of community care, the commitment offense for each program participant, and annual expenditures for each facility and program contractor. In addition, the department should report on the status of any ongoing evaluations of CDC substance abuse programs.
We recommend approval of the request for $5.1 million for additional security equipment. We further recommend modifying the proposal to eliminate changes to operational policies in the Security Housing Unit and Administrative Segregation Unit because these changes may have unintended consequences and result in increased costs.
Background. The CDC currently provides the following types of inmate housing:
Budget Proposal. The budget proposes $8.4 million to implement the Violence Control Pilot Program (VCP), a continuum of housing and program settings for male inmates. This continuum includes reduced privileges in both SHU and ASU, and a new Basic General Population (BGP) program for inmates being released from SHU. The purpose of this program is to create an interim setting between SHU/ASU and TGP. The program would include a system of incentives and penalties designed to discourage inmates from violent behavior so inmates can leave SHU or ASU and transition back to the TGP.
According to the proposal, BGP inmates would enter the program with fewer privileges than inmates in the existing TGP. The program would provide BGP inmates with increased supervision and life skills training, such as anger management and conflict resolution classes. Inmates would earn additional privileges by participating in prescribed programs and refraining from violent behavior. The program, which consists of five steps of progressively increasing privileges, would transition inmates into the TGP in about 18 months. Concurrently, inmates in SHU and ASU would have fewer privileges than are currently provided and would receive basic levels of care mandated by law, including housing, food, education, and medical care.
In addition to providing support for the VCP, the proposal includes $5.1 million for security equipment for all correctional officers at maximum security prisons.
Program May Have Unintended Effects. The proposal indicates that the main purpose of the VCP is to reduce the level of violence in TGP caused by inmates released from SHU. However, the proposal also includes two significant policy changes to the operation of the SHU and ASU units which could potentially increase the level of inmate violence in those housing units for reasons discussed below. The first policy change would be to shift SHU lengths of stay from determinate to indeterminate time frames. This would mean that, regardless of the SHU offense, each inmate would require a review at each minimum eligibility release date. The second policy change is the curtailment of already reduced privileges, such as telephone calls and canteen purchases.
The proposal indicates that these policy changes will create a disincentive for SHU and ASU inmates to engage in violent behavior. The department, however, has not provided any evidence to support the claim that inmates engage in less violent behavior when privileges are reduced. For example, the department could provide no evidence that inmates in housing units with fewer privileges, such as SHU and ASU, are involved in fewer violent incidents than inmates in the TGP. In fact, past departmental budget proposals for additional resources for restrictive housing units have indicated that SHU and ASU inmates are involved in more violent incidents that TGP inmates. Therefore, it is possible that a further reduction in privileges could have no change or even increase violent inmate behavior in these restrictive housing units, resulting in a need for additional security resources in the future. In addition, the conversion of terms for inmates in SHU from determinate to indeterminate time frames could cause inmates to be housed at a higher security level for longer than necessary, thereby adding to the existing shortage of SHU and ASU housing.
Analyst's Recommendation. We recommend the Legislature approve the request for $5.1 million to provide correctional officers with additional security equipment. However, we recommend modifying the proposal to eliminate the reduction of privileges in SHU and ASU and the conversion of SHU terms to indeterminate time frames to avoid unintended program consequences and potential higher costs. This modification will not affect the operation of the BGP portion of the proposal.
We recommend the California Department of Corrections report to the Legislature prior to budget hearings on how the department can implement reforms to improve service delivery and reduce costs associated with pharmacy services and medical contracting.
We recommend approval of $16 million proposed to increase inmate access to medical care at four prisons, as well as $8 million proposed to allow the department to use an outside contractor to procure mental health staff.
We withhold recommendation on the proposed $82.8 million augmentation for pharmaceuticals and medical contracting pending a report at budget hearings on how the department intends to reduce costs associated with pharmacy services and medical contracting. We also withhold recommendation on a proposal to increase mental health crisis beds and psychiatric services unit beds at California State Prison, Sacramento pending receipt of a report from the department explaining discrepancies in the budget proposal regarding the number of needed beds.
Budget Proposal. The budget proposes several augmentations to the CDC Health Care Services Division (HCSD) programs. The augmentations total over $117 million, which is almost three times the increase approved in the 2000-01 Budget Act. About 70 percent, or $82.8 million, of this amount is for pharmacy and contract medical services. The remaining $34 million is for proposals to do the following.
Background. The HCSD is responsible for the management and provision of medical care for state prison inmates. In January 2000, a Bureau of State Audits (BSA) report commissioned by the Legislature found that the department did not adequately use many standard managed care practices that could help hold down CDC's medical costs.
In particular, BSA found that CDC used only limited methods to contain costs and ensure uniform care. As a result, medical operating costs varied widely among prisons. The BSA also determined that rapidly growing CDC pharmacy costs could be reduced if the department employed more effective contracting methods.
The 2000-01 Budget Act appropriated over $41 million to help CDC move closer to compliance with the findings of the BSA audit and a federal court order to improve mental health services to inmates requiring higher security. Specifically, CDC reforms included establishing a team to audit the quality of care at each prison, implementing a system to track inmate appeals on health care issues, removing barriers to medical delivery through policy changes, and conducting a feasibility study to determine if an outside entity would be able to direct and operate a correctional managed health care system. The budget act also appropriated funds for increased medical contracting and supply costs and to improve the health care utilization management unit.
Analyst's Recommendations. Below, we summarize our recommendations for CDC's budget proposals for its medical operations.
We recommend the Legislature approve a request for $21.8 million to fund the California Department of Correction's (CDC) increased workers' compensation costs.
We withhold recommendation on $36.6 million proposed for relief staffing pending a report from CDC at budget hearings on how the department plans to reduce high levels of accumulated staff leave and ensure that posted staff will utilize sufficient leave time to justify full relief staffing.
The Governor's budget proposes $58.4 million to address several of CDC's personnel management issues, some of which were highlighted by two BSA reports on CDC's personnel management practices. In this analysis, we provide an update on the department's progress in implementing reforms, discuss the personnel management proposals in the Governor's budget, and make recommendations for legislative action.
Background. In recent years, we have pointed out that CDC has had significant problems in effectively managing its prison staff personnel. Most recently, in the Analysis of the 2000-01 Budget Bill, we discussed the findings of the BSA reports which indicated that poor prison personnel management practices were costing the state as much as $35 million annually and building up a state financial liability to compensate for leave time accrued by departmental staff. We estimate this liability could amount to $127 million by 2004.
The first BSA audit, released in July 1999, found that CDC improperly authorized overtime for its employees. The most recent audit, released in late January 2000, concluded that CDC had failed to effectively manage sick leave usage and its holiday and leave programs. As a result, the department was incurring high overtime costs primarily as a result of some custodial staff having to backfill for other custodial staff who were out on sick leave. Both audits recommended reforms for CDC personnel management practices.
Recent information from CDC indicates it has taken steps to improve its personnel management practices. The department, however, continues to experience significant amounts of leave liability and as well as increases in workers' compensation expenditures, as we discuss below.
The CDC Personnel Management Practices Update. Although CDC has started to implement some of the reforms proposed in the BSA audit, the department has not experienced significant reductions in personnel costs. In this section, we provide an update on the department's progress in implementing various personnel reforms and identify areas which continue to need improvement.
At the time this analysis was prepared, CDC's new overtime management policies seemed to have had limited, if any, impact. Available data indicate that overtime use continues to increase and the department expects current overtime expenditures to increase to $217 million, which represents a 35 percent increase during the two-year period since 1999-00.
Several Components to Personnel Augmentations. The most significant increase in the personnel budget is $36.6 million to maintain sufficient relief staff levels, allowing regular custody staff to use all earned vacation and sick leave. This augmentation is intended to prevent staffing deficiencies resulting from staff taking earned leave and minimize the department's use of overtime to fully staff all posted positions.
The Governor's budget also proposes $21.8 million to fund prior-year budget shortfalls in the workers' compensation budget. In addition to this augmentation, the department proposes to redirect two positions to impose cost control measures on the program by tracking, monitoring, and analyzing workers' compensation data.
The CDC Proposals Have Some Weaknesses. Our analysis of the CDC personnel management proposals identifies several problems that could weaken their effectiveness in reducing and/or controlling personnel costs.
Analyst's Recommendation. Despite the concerns raised by the BSA audits regarding mismanagement of personnel operations at state prisons, it appears that corrective action taken by CDC during the current year has not resulted in significant improvement or cost reduction. Accordingly, we recommend that the Legislature:
We recommend a reduction of $3.1 million requested in the California Department of Corrections' budget for cadet and parole agent academy salary increases, information technology backlog maintenance, training simulation staff, the headquarters consolidation project, and facility planning. (Reduce Item 5240-001-0001 by $3.1 million.)
The CDC budget proposes funding increases relating to cadet and parole agent academy salary increases, information technology backlog maintenance, training simulation staff, the headquarter's consolidation project, and facility planning.
Analyst's Recommendation. We recommend deletion or a reduction of funding for various proposed expenditures that our analysis indicates are not justified, and offer other recommendations as outlined below.