LAO Contact

March 23, 2020
COVID-19
Covid-19: Federal Health-Related Response
Updated June 1, 2020 to reflect the April 24th enactment of H.R. 266, the Paycheck Protection and Health Care Enforcement Act, and includes updates through May 28 to prior federal actions discussed previously in the post.
Updated May 6, 2020 to reflect revised estimates of the fiscal impact of enhanced federal Medicaid funding available through the Families First Coronavirus Response Act.
Updated April 7, 2020 to reflect the state’s intention to cover COVID-19 testing for the uninsured through Medi-Cal.
Updated April 4, 2020 to reflect the March 27th enactment of H.R. 748, the Coronavirus Aid, Relief, and Economic Security (CARES) Act, and include updates to prior federal actions discussed previously in the post.
This updated post highlights key federal actions in response to coronavirus disease 2019 (COVID-19)—through May 28, 2020—relating to public health broadly and individual health care. While this post reflects our best understanding of the high-level content and implications of the federal actions and, where applicable, state responses to them to date, we will continue to update the post as new information and clarifications become available, and as additional federal actions are taken.
This post highlights the health-related features and implications of five major sets of federal actions that provide significant funding directly to state/local health agencies and/or have significant programmatic implications for the delivery of the state’s health care and public health activities. These five sets of actions are:
The passage of legislation signed on March 6 providing funding largely for public health infrastructure.
The declaration of a national emergency on March 13 that, among other things, activates assistance from the Federal Emergency Management Agency (FEMA) for activities directed by public health officials, as well as opens the door for states to apply for increased flexibility in the delivery of Medicaid services.
The passage of legislation signed on March 18 that, among other things, provides a temporary increased federal share of cost for Medicaid services and funding to provide universal coverage of COVID-19 testing without cost sharing.
The passage of legislation signed on March 27 that, among other things, provides funding for public health infrastructure, hospitals and other health care providers, and behavioral health services, and makes changes to private health insurance coverage for COVID-19 testing and treatment.
The passage of legislation signed on April 24 that, among other things, provides additional funding for health care providers to help cover expenses or lost revenues associated with their response to COVID-19 and additional funding for testing.
Coronavirus Preparedness and Response Supplemental Appropriations Act (CPRSAA)
The President signed H.R. 6074, the CPRSAA, into law on March 6, appropriating $8.3 billion for various COVID-19-related activities, including $6.2 billion for the U.S Department of Health and Human Services (DHHS). These DHHS funds are less for individual testing and treatment (which are addressed in a second federal package discussed later in this post) and more for public health infrastructure—lab capacity, staffing, surveillance (the systematic collection and analysis of health-related data), epidemiology (which, in this context, refers to assessments of near- and long-term COVID-19 health outcomes to guide decision making), medication and vaccination development and purchase, medical supplies, and health provider training. In addition, this new law waives restrictions on billing for telehealth services provided to Medicare beneficiaries.
Funding for State and Local Entities Nationwide Through the Centers for Disease Control and Prevention (CDC). The CDC received $2.2 billion of the DHHS total, of which $950 million was for grants to and cooperative agreements with states, localities, tribes, and territories. This funding augmented initial transfers from DHHS to the CDC totaling $35 million. The COVID-19 funding supports a variety of public health preparation and response activities, including surveillance, epidemiology, increased lab capacity, infection control, communications, and mitigation efforts. This particular funding cannot be used for research or clinical care. The amounts provided to state and local governments are based in large part on their existing Public Health Emergency Preparedness grants with the CDC. Certain recipients have also received a supplemental payment, including both the state and Los Angeles County (which receives CDC funding directly from the federal government).
California Received $90.7 Million From the CDC Through DHHS Transfers and the CPRSAA. The State of California and Los Angeles County have received CDC funding totaling $90.7 million from the DHHS transfers and the CPRSAA, as described below. (We note that additional CDC awards will be made with funding from a subsequent legislative package signed on March 27, discussed later in this post.)
State of California via California Department of Public Health (CDPH): $63.3 million.
$59.7 million based on CDPH’s existing cooperative agreement with the CDC and including a supplemental payment.
$2.6 million from the CDC’s Emerging Infections Program.
$1 million from the CDC’s Epidemiology and Laboratory Capacity program.
-
Los Angeles County: $27.4 million.
$26.4 million based on CDPH’s existing cooperative agreement with the CDC and including a supplemental payment.
$1 million from the CDC’s Epidemiology and Laboratory Capacity program.
Majority of CDC Funding to State Will Be Passed Through to Local Health Jurisdictions. When the state receives CDC Public Health Emergency Preparedness grants, CDPH typically distributes at least 70 percent of the funding to local health jurisdictions and retains 30 percent for state operations. The same is true in this case—of the $59.7 million provided to CDPH based on its cooperative agreement and supplemental payment, $42.3 million is being provided to local health jurisdictions for local activities (not including Los Angeles County, which is receiving direct grant funding from the CDC), while $17.4 million will go for statewide activities. The state also received separate payments for surveillance through the CDC’s Emerging Infections Program and for epidemiology and lab capacity through the CDC’s Epidemiology and Laboratory Capacity program.
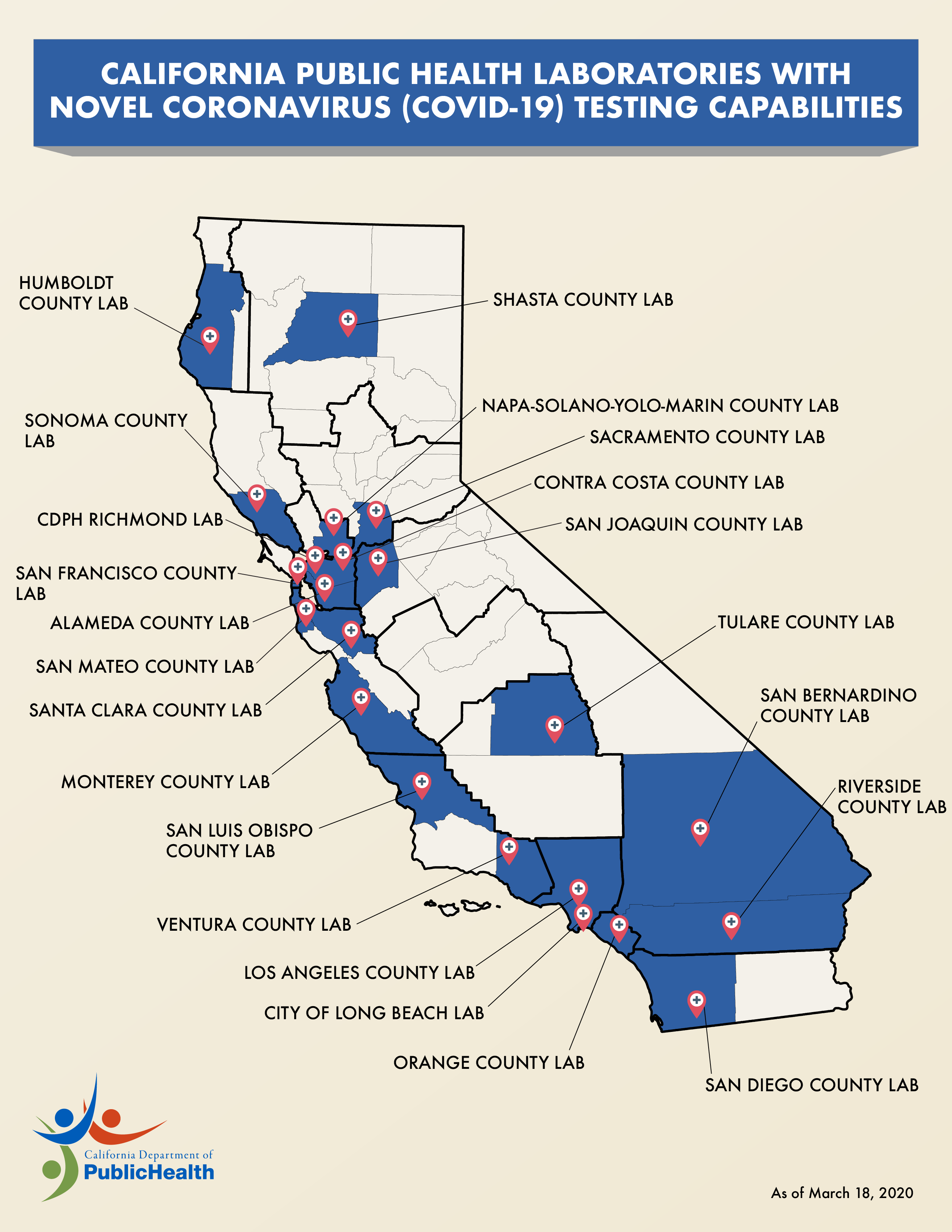
Current Public Health Efforts. The CDPH and California’s 61 local health jurisdictions have been conducting surveillance and managing testing, communications, preparedness, and response. Testing is being conducted at 22 state and county public health labs and at all five University of California (UC) Medical Centers. Private labs are conducting testing as well. CDPH maintains a website with information about COVID-19, including the latest facts and figures, as well as guidance for various groups—health providers, first responders, long-term care facilities, homeless shelters, schools, food and beverage businesses, and individuals and households. CDPH is also working closely with the Governor to design a pandemic roadmap to lay out steps for a phased reopening of the state.
{kind=link}
Remaining Federal Funding Supports National Efforts, With State and Local Implications. While the remaining DHHS funding in CPRSAA is not provided directly to states and localities necessarily, the benefit ultimately should be widespread. For example, $836 million is for the National Institute of Health’s National Institute of Allergy and Infectious Diseases for research to prevent and treat coronavirus. Another $3.1 billion is for the Public Health and Social Services Emergency Fund to develop and purchase vaccines and to procure necessary medical supplies, therapeutic medications, and diagnostic tests.
National Emergency Declaration
When the President declared a national emergency on March 13, it increased federal support for DHHS and authorized the Secretary of Health and Human Services (HHS) to waive certain health care delivery requirements, as described below. It also activated the assistance of FEMA, which is working under the overall direction of DHHS. (We describe federal assistance as a result of the national emergency declaration and implications for California in another post.) From a public health perspective, the activation of FEMA and its local field offices allows it to assist states, local governments, tribes, and territories with their emergency response efforts, including by procuring supplies and paying for certain eligible activities—at a 75 percent federal share of cost—that are undertaken at the direction of public health officials (so long as another funding source is not available for that activity).
Additional Flexibility for Medi-Cal Service Delivery
States May Seek Flexibility in How Medicaid and Children’s Health Insurance Program (CHIP) Services Are Delivered. When the President declares an emergency and the federal Secretary of HHS declares a public health emergency, the HHS Secretary is authorized to waive various requirements of the Medicare, Medicaid, and CHIP programs for the purpose of ensuring access to needed health care services. A major mechanism for obtaining such new flexibilities is through 1135 waiver authority, which is available for the duration of the emergency. For Medicaid and CHIP programs, states generally must submit a request to the federal government to waive program requirements.
California Has Applied for 1135 Waiver Authority Seeking Broad Programmatic Flexibility. Medi-Cal, California’s combined Medicaid and CHIP program, is administered by the Department of Health Care Services (DHCS). In March and April 2020, DHCS submitted three separate 1135 waiver requests to the federal government to waive a large number of federal Medicaid and CHIP requirements in an effort to ensure and improve access to Medi-Cal services during the emergency period. In addition, under the guidance of the federal government, DHCS has submitted requests for certain flexibilities through other federal authorities, such as the state’s 1115 waiver and state Medicaid plan amendments.
Federal Government Has Partially Approved California’s Requests for New Flexibilities. Since March 23, 2020, the federal government has approved a number of DHCS’s requests for temporary Medi-Cal flexibilities. In its most recent approval letter, the federal government communicated to DHCS that it continues to process the state’s requests that have yet to be approved. Accordingly, the federal government may approve additional Medi-Cal flexibilities in the coming weeks. In addition, the federal government has issued other forms of guidance that provide flexibilities to state Medicaid programs, such as “blanket waivers” of federal Medicare law. The flexibilities offered through these blanket waivers apply, at least partially, to Medi-Cal.
The following bullets highlight a number of the major programmatic flexibilities that DHCS sought through its initial 1135 waiver requests, and indicate if they have been approved or a federal decision remains pending:
-
Approved: Streamline Provider Enrollment. In order to be reimbursed by Medi-Cal, health care providers must enroll in the program. To enroll, providers must meet a number of requirements. DHCS requested to waive several of these requirements, such as passage of a fingerprint-based background check and in-state licensure as a health care professional. Waiver of the latter requirement allows, for example, physicians licensed in other states to come to California and receive reimbursement for the Medi-Cal services they deliver.
-
At Least Partially Approved: Provision of Services in Alternative Settings. Many Medi-Cal services are only reimbursed if they are provided within certain health care settings or facilities, such as doctor’s offices and hospitals. DHCS requested to allow providers to be reimbursed for services provided in alternative settings, such as mobile testing sites and temporary shelters (for example, converted hotels). The federal government has at least partially approved this request, specifically approving reimbursement for various kinds of long-term services and supports (such as care in nursing facilities and in-home personal care services) provided in alternative settings. Recently released federal blanket waivers may extend this approval to additional provider types as well, such as hospitals, providing Medi-Cal services in alternative settings.
Partially Approved: Stop Requiring Prior Authorization. Many Medi-Cal services require administrative review—known as prior authorization—before being delivered and reimbursed. For example, many expensive prescription drugs require prior authorization. DHCS requested to waive all prior authorization requirements in Medi-Cal in order to prevent delays in access to needed services and medical products. The federal government has partially approved this request—approving the waiver of prior authorization requirements in Medi-Cal’s fee-for-service (FFS) but generally not in Medi-Cal’s other delivery systems. However, the federal government gave the authority to the states to decide whether Medicaid managed care plans may waive prior authorization for the testing and treatment of COVID-19. DHCS has exercised this authority. As a result, Medi-Cal managed care plans may not require prior authorization of COVID-19 testing and treatment. Whether the federal government may approve additional waivers of prior authorization requirements in Medi-Cal delivery systems other than FFS is unclear.
-
Approved: Removal of 100-Day Supply Limit on Prescription Drugs. Pharmacies are limited to dispensing up to a 100-day supply of prescription drugs to Medi-Cal beneficiaries. DHCS requested to waive this limit and thereby allow beneficiaries to obtain larger supplies of prescription drugs.
-
Generally Approved: Broaden Allowable Use of Telephonic Assessments and Telehealth Visits. Many Medi-Cal services are authorized only to be delivered in certain physical settings. DHCS proposes to waive such requirements to allow providers to (1) telephonically assess beneficiary eligibility for certain services (such as In-Home-Supportive Services) and (2) deliver services virtually (for example, a doctor’s visit at a Federally Qualified Health Center). DHCS requested that payment rates for telehealth visits be equivalent to in-person visits. While the federal government generally has not directly responded to the state’s request to broaden the allowable use of telehealth in Medi-Cal, other forms of federal guidance, such as blanket waivers, provide significant new flexibilities in this area, which we understand generally apply to Medi-Cal. DHCS has issued guidance outlining these new telehealth flexibilities, which include, for example, making payment rates equivalent for in-person and telehealth services.
-
Approved: Expand Eligibility for Hospital Presumptive Eligibility. Hospitals currently are authorized to presume that patients are eligible for Medi-Cal, and thereby receive Medi-Cal reimbursement, based on preliminary patient information indicating potential Medi-Cal eligibility. However, hospital presumptive eligibility is only available for certain types of potential Medi-Cal enrollees. For example, seniors and persons with disabilities are not eligible for this presumptive eligibility. DHCS requested to expand hospital presumptive eligibility to additional types of Medi-Cal enrollees, including seniors and persons with disabilities and uninsured individuals not normally eligible for Medi-Cal but who are allowed under federal COVID-19-related legislation to receive Medicaid coverage at states’ option. In addition, individuals generally only are eligible for enrollment through hospital presumptive eligibility once per year. DHCS requested to waive this limitation.
Approved: Waive Share of Cost for COVID-19-Related Services. Certain Medi-Cal beneficiary populations must pay a share of cost for Medi-Cal services before Medi-Cal will pay for the remaining cost of the services they receive. DHCS requested to waive these beneficiaries’ share of cost for COVID-19-related services, including testing, diagnosis, and treatment.
-
Approved: Increase Certain Provider Payments. DHCS requested to increase a number of provider payments, such as long-term care facility payment rates—to help these facilities cope with higher costs resulting from COVID-19 and clinical laboratory payment rates—to help these facilities process the significant and growing number of COVID-19 tests.
-
Pending: Allow Federal Reimbursement for Institutions for Mental Disease (IMDs). IMDs are health facilities with more than 16 beds that primarily treat mental illness and substance use disorders. The federal government, through Medicaid, generally will not pay for services in IMDs. DHCS requested to waive this limitation so that the state can receive federal reimbursement for IMD services, which could help IMDs temporarily expand capacity as needed.
Families First Coronavirus Response Act (FFCRA)
On March 18, the President signed H.R. 6201, FFCRA, which includes additional actions and federal funding to address the COVID-19 outbreak. In this section, we focus on two health-related items in FFCRA—(1) a temporary increase to the federal share of cost in Medicaid and (2) provisions to require universal coverage of COVID-19 testing without cost sharing. (We describe other FFCRA provisions in other posts.)
Enhanced Federal Funding for Medi-Cal
FFCRA Temporarily Increases Federal Funding for Medi-Cal by 6.2 Percentage Points. Medicaid is an entitlement program whose costs generally are shared between the federal government and states based on a set formula. To relieve state budgetary pressure caused by COVID-19’s likely impacts on state Medicaid expenditures and tax revenues, Congress approved a temporary 6.2 percentage point increase in the federal government’s share of cost for state Medicaid programs. For most Medi-Cal beneficiaries and services, the federal government pays 50 percent of Medi-Cal costs. Under FFCRA, beginning January 1, 2020 and ending the first quarter in which the COVID-19 public health emergency is not in effect, the federal share of cost for those Medi-Cal beneficiaries and services will increase from 50 percent to 56.2 percent. Because Medicaid is an entitlement program, the amount by which federal funding will increase is not limited to a fixed appropriation and instead will vary based on Medi-Cal beneficiary-eligibility levels and overall program costs.
To Receive Enhanced Federal Funding, the State Must Comply With a Set of New Federal Requirements. FFCRA places a set of conditions on states in order for them to receive the enhanced federal funding. To qualify for the funding enhancement, the State of California may not:
Make changes to Medi-Cal eligibility rules and procedures that are more restrictive than those in place as of January 1, 2020.
Charge higher premiums than were in place as of January 1, 2020.
Impose cost sharing for COVID-19 testing, services, and treatments.
Terminate coverage for Medi-Cal members who were enrolled in the program on or after March 18, 2020 unless the member (1) moves out of state, (2) voluntarily disenrolls, or (3) is deceased.
Increase local governments’ share of cost—in percentage terms—for Medi-Cal expenditures.
Potential Fiscal Impact of Enhanced Federal Funding for Medi-Cal. Significant federal, state, and local funding flow through Medi-Cal in California. Based on assumptions in the Governor’s January budget (prior to the COVID-19 outbreak), we estimated that total funding for Medi-Cal will be roughly $113 billion in 2019-20, including $66 billion from federal funds, $30 billion from the state General Fund, $8 billion from other state funds, and $9 billion from local funds. This includes funding for DHCS, as well as funding for programs administered by other agencies that are funded through Medi-Cal.
The overall net fiscal impact to the state of the enhanced federal funding is subject to considerable uncertainty. Based on preliminary LAO estimates that incorporate changes in caseload and costs as a result of COVID-19, the enhanced federal funding could potentially reach between $400 million and $500 million per month (while the enhancement remains in effect)—which reflects nearly 5 percent of average total monthly spending on the major state HHS programs that are funded through Medi-Cal. Most of this $400 million to $500 million per month would directly offset state General Fund spending in Medi-Cal, as well as in the In-Home Supportive Services and Department of Developmental Services programs that rely on Medicaid funding. The portion of increased federal funding that does not directly offset state General Fund spending largely would offset a share of Medi-Cal costs that are paid by other entities such as counties and hospitals.
Our preliminary estimates project that the enhanced federal funding will result in significant General Fund savings on a state fiscal-year basis. Assuming, for example, that the enhancement is in place through December 31, 2021,we project that the state would receive General Fund savings of almost $2 billion in 2019-20, around $4 billion 2020-21and around $2 billion in 2021-22.
Estimated Savings Likely Will Be Only Partially Offset by Higher Medi-Cal Costs as a Result of COVID-19. The COVID-19 pandemic is likely to cause significantly higher Medi-Cal costs in the near term, particularly due to higher enrollment in the program as a result of the deteriorating economic environment and FFCRA requirement that prohibits the state from disenrolling existing enrollees even if they do not meet most eligibility requirements. Higher overall costs in Medi-Cal could also result from testing, treating, and vaccinating against COVID-19. Preliminarily, we project that the higher caseload and utilization costs associated with COVID-19 likely will only partially offset the savings from the enhanced federal funding.
Accelerating Medi-Cal Payments Could Maximize the Use of Enhanced Federal Funding. A Medi-Cal payment will be eligible for enhanced federal funding as long as the payment to the Medi-Cal provider is made during the period of eligibility for enhanced federal funding. Accordingly, a Medi-Cal service that occurs during the national emergency period, but for which payment occurs after the period of eligibility for enhanced federal funding ends, will not receive enhanced federal funding. Medi-Cal payments often occur months after the provision of services. Accelerating Medi-Cal payments to ensure they occur during the period of eligibility for enhanced federal funding would maximize federal funding for Medi-Cal and help relieve pressure on the General Fund resulting from COVID-19. Around the time of the Great Recession, the state took some actions to achieve this very purpose—specifically, speeding up some FFS payments temporarily. Similar and additional actions could be considered now. In addition, the Legislature could consider asking DHCS for recommendations on measures that could be put in place to accelerate Medi-Cal payments without creating undue burden on providers.
Universal Coverage of COVID-19 Testing Without Cost Sharing
FFCRA includes provisions to ensure that all individuals who need to be tested to learn if they have contracted COVID-19 will not be required to pay anything out of pocket for the testing while the public health emergency is in effect, regardless of whether they have health insurance or the source of their insurance coverage. FFCRA accomplishes this in a few main ways. (Subsequent congressional action builds on these provisions, as we describe later.)
Private and Public Insurance Required to Cover Testing Without Cost Sharing. First, FFCRA requires all private health insurers to cover the cost of COVID-19 testing without any required cost sharing, such as deductibles or copayments, on the part of the individual enrolled in coverage. In other words, individuals with private health insurance cannot be separately charged (beyond regular premium payments to maintain insurance coverage) to be tested. Furthermore, private insurers cannot require individuals to wait for prior authorization by the insurer before being tested. FFCRA also places these requirements on public insurance coverage programs, such as Medicare (the federal health insurance program for the elderly and disabled) and Medicaid (the state-federal low-income health insurance program, known as Medi-Cal in California).
States Optionally May Cover Uninsured in Medicaid for Purposes of Testing. To address COVID-19 testing for those without coverage, FFCRA gives states the option to enroll uninsured individuals in Medicaid for purposes of COVID-19 testing only. While Medicaid costs typically are shared by states and the federal government, the federal government will cover 100 percent of the costs of providing COVID-19 testing to this population through Medicaid. As of the writing of this post, California had not yet made a determination on whether or not to cover COVID-19 testing for the uninsured through Medi-Cal.
Funding to Cover Cost of Testing for Uninsured Individuals. Additionally, for individuals who are uninsured and do not otherwise have coverage for COVID-19 testing (such as if a state chooses not to cover such testing through Medicaid), FFCRA provides up to $1 billion to reimburse health care providers for tests performed for such individuals. This funding would flow to health care providers through the federal National Disaster Medical System.
Coronavirus Aid, Relief, and Economic Security (CARES) Act
The President signed H.R. 748, the CARES Act, into law on March 27, appropriating over $2 trillion for COVID-19-related activities and related financial relief. In this section, we provide details of the health-related provisions of the CARES Act. These include provisions that provide funding for public health infrastructure, hospitals and other health care providers, and behavioral health services, and make changes to private health insurance coverage for COVID-19 testing and equipment.
Funding for Public Health Infrastructure
CDC Funding for State and Local Entities. The CARES Act provides the CDC with an additional $4.3 billion, available until September 30, 2024. (As noted above, previous federal action—enactment of CPRSAA—provided the CDC with $2.2 billion.) About one-third of the additional CDC funding ($1.5 billion) is for grants to and cooperative agreements with states, localities, tribes, and territories. As with the previous allocations to state and local governments, this funding will support a variety of public health preparation and response activities, including surveillance, epidemiology, increased lab capacity, infection control, communications, and mitigation efforts.
CDC CARES Act Funding for State and Local Governments Includes at Least $62.1 Million for California. Both the State of California and Los Angeles County will receive CDC CARES Act grants. The CARES Act calls for these grants to be, at minimum, the same amount provided through 2019 Public Health Emergency Preparedness (PHEP) grants. Including CDC funding from initial HHS transfers, CPRSAA, and the CARES Act, California will receive a total of at least $152.8 million from the CDC for public health infrastructure, broken out as follows:
-
State of California via CDPH: $105.2 million.
$63.3 million from CPRSAA (H.R. 6074) funding and U.S. DHHS transfers.
$41.9 million from initial CARES Act (H.R. 748) funding.
-
Los Angeles County: $47.6 million.
$27.4 million from CPRSAA (H.R. 6074) funding and U.S. DHHS transfers.
$20.2 million from initial CARES Act (H.R. 748) funding.
While additional CDC CARES Act grants ultimately may become available to state and local governments, details about these grants and guidance for accessing these funds have not been provided yet.
States Can Request Supplies From the Strategic National Stockpile. The Strategic National Stockpile is the national supply of pharmaceuticals and medical supplies that can be accessed by state and local governments during public health emergencies when there is a shortfall in local supplies. Each state has a specific plan for how to request supplies from the stockpile; in California, health facilities are directed to contact their Medical Health Operational Area Coordinator or local public health officer. The CARES Act adds language to the federal law governing the stockpile to include the following specific examples of stockpile contents: personal protective equipment; ancillary medical supplies; and other supplies that are needed to administer drugs, vaccines and other biological products, medical devices, and diagnostic tests. It also provides up to $16 billion through the Public Health and Social Services Emergency Fund (PHSSEF) to sustain the stockpile. In the course of responding to the COVID-19 pandemic, California already has made multiple requests for personal protective equipment (PPE) and other supplies from the Strategic National Stockpile and has received some shipments. California also has made efforts to procure its own face masks—both N95 and surgical masks—by contracting directly with manufacturers. Large influxes of PPE are expected to arrive in May and June. The state is trying to meet the current demand for PPE among the health care workforce and patient population, but also among other sectors as the state begins to reopen.
Additional Public Health-Related CARES Act Funding Will Benefit California. The CARES Act includes funding for poison control centers (California’s Emergency Medical Services Authority is receiving $572,000 for this purpose) and for the Ryan White HIV/AIDS program. Of the latter appropriation, California is receiving $9.1 million—$1.5 million to supplemental an existing CDPH grant, $4 million for programs run by cities and counties, $1.1 million for UC Medical Centers, and $2.5 million for other nonprofits and clinics. The CARES Act also includes funding for other activities that will benefit California’s public health, either as direct grants or reimbursements to California or indirectly, such as by way of vaccine and medication development. For example, the National Institutes of Health will receive $945 million for research and related activities. PHSSEF may be used to provide grants to state or local governments to construct or renovate nonfederal facilities to improve preparedness or response capabilities. At least $3.5 billion from PHSSEF is for the manufacture, production, and purchase of vaccines, therapeutics, diagnostics, and pharmaceutical ingredients. PHSSEF funds also may be used to enhance and protect the U.S. medical supply chain and at least $250 million is available for the Hospital Preparedness Program.
Funding for Hospitals, Safety Net Clinics, and Other Health Care Providers
$100 Billion in Relief Funding for Hospitals and Other Health Care Providers. The CARES Act establishes the Provider Relief Fund (PRF), which makes available $100 billion in funding nationwide for hospitals and other health care providers that provide diagnosis, testing, or care for individuals who have COVID-19 or are suspected of having COVID-19. This funding may be used for a variety of purposes, such as leasing properties, setting up temporary structures for treatment activities, retrofitting facilities, purchasing medical supplies and equipment, and bringing on and training additional health care workers. The funding also may be used to offset lost revenues resulting from the COVID-19 outbreak, such as those associated with hospitals cancelling elective procedures to free up capacity to address the COVID-19 outbreak. The federal government has elected to allocate this funding in multiple rounds according to different methodologies and priorities. To our knowledge, about $3.9 billion from PRF has been distributed to California health care providers as follows:
$2.9 Billion to California Health Care Providers Based on Share of Medicare FFS Volume. Initially, $30 billion from PRF was distributed to health care providers nationwide based on their share of Medicare FFS reimbursements. About $2.9 billion of this distribution went to health care providers in California.
Additional Allocation Made to Augment Providers’ Share of Distribution. Another $20 billion from PRF has been distributed to health care providers nationwide such that the total amount for the first two rounds of funding ($50 billion) is allocated based on providers’ share of net patient revenue from all sources. The amount of this distribution that went to California health care providers is unknown.
$356 Million for California Skilled Nursing Facilities (SNFs). $4.9 billion from PRF will be distributed nationwide to SNFs. About $356 million of this funding will go to SNFs in California.
$325 Million for California Hospitals That Treated a High Number of COVID-19 Patients. $12 billion from PRF will be distributed nationwide to hospitals that provided inpatient care to 100 or more COVID-19 patients through April 10, 2020. An additional $2 billion from PRF will also be distributed to these hospitals based on the amount of care they provide to low income and uninsured patients. About $325 million of this funding will go to hospitals in California.
$300 Million for California Health Care Providers in Rural Areas. $10 billion from PRF will be distributed nationwide to hospitals and other providers located in rural areas. About $300 million of this distribution will go to hospitals and other providers in California.
Allocation Made to the Indian Health Service and Tribal Providers. $500 million from PRF will be distributed to the Indian Health Service and tribal hospitals, clinics, and health centers. The amount of this distribution that will go to tribal providers in California is unknown.
Details About Upcoming Allocations Are Pending. Details about how the federal government will allocate the remaining $22.6 billion from the initial amount provided for PRF under the CARES Act have not yet been announced. (We discuss an additional $75 billion provided to PRF later in this post under our section on “COVID Phase 3.5”.) However, DHHS has indicated that some of the remaining funding will be distributed to other provider types such as dentists or providers that solely accept Medicaid patients or that treat uninsured patients.
Increases Funding for Health Centers. Health centers are a major provider of safety net primary care services in California. A significant portion of health center funding comprises grants from the federal government. This federal grant funding was set to expire in May 2020. The CARES Act extends this funding through November 2020. The CARES Act also provides an additional $1.32 billion nationwide for health centers for the prevention, detection, and treatment of COVID-19. Of this $1.32 billion, California-based health centers received $193 million in additional funds. In addition, FFCRA previously provided $100 million in federal funding nationwide for health centers. Of this $100 million, California-based health centers received nearly $14 million in additional funds.
Funding for Behavioral Health Services
Funding for Behavioral Health Nationwide Through the Substance Abuse and Mental Health Services Administration (SAMHSA). The CARES Act includes $425 million to SAMHSA for mental health and substance use programs to respond to the COVID-19 outbreak, most of which is available as grant funding for states or local entities. This funding is allocated as follows:
$250 Million for the Certified Community Behavioral Health Clinics (CCBHC) Expansion Grant Program. CCBHCs are a distinct provider type in the Medicaid program that offer a comprehensive set of mental health and substance use services to beneficiaries with high needs. CCBHCs receive an enhanced Medicaid reimbursement rate based on anticipated costs of offering services. Currently, eight states operate in the federal CCBHC Demonstration Program. In 2016, California received planning grant funding from SAMHSA to prepare for this demonstration program, but was not one of the states ultimately selected. Under the CCBHC Expansion Grant Program, either the state, individual CCBHCs, or clinics that can obtain CCBHC certification in a short amount of time are eligible to apply for federal grant funding to expand services provided. It is our understanding that the state is not planning to pursue this funding opportunity at this time, although individual clinics can still choose to apply. However, how many clinics in California can meet the application requirements at this time is unknown.
$100 Million for Behavioral Health Emergency Response Grants. The CARES Act includes $100 million available to state or local entities nationwide as noncompetitive emergency grant funding to address emergency mental health or substance use needs, including resources for targeted populations such as youth or homeless individuals. Of this amount, $2 million was allocated to California.
$50 Million for Suicide Prevention Efforts. The CARES Act includes $50 million in grant funding available to state entities, local entities, or individual behavioral health providers to support suicide prevention programs. What amount of this funding will be allocated to California is unknown.
$15 Million for Tribal Behavioral Health Services. The CARES Act also makes available $15 million nationwide to support tribal behavioral health services. Of this amount, about $2 million was allocated to tribal organizations in California.
Insurance Coverage Requirements for COVID-19 Testing and Treatment
Changes to Private Health Insurance Coverage Requirements for COVID-19 Testing and Treatment. As described above, FFCRA imposes requirements on private health insurers to cover the cost of COVID-19 testing without cost sharing. The CARES Act builds on these requirements in a few ways. Specifically, the CARES Act:
-
Broadens requirement that private health insurers cover COVID-19 testing, with no cost sharing, to include tests that have requested emergency use approval from the Food and Drug Administration, tests developed by states, and any other tests the U.S. DHHS determines to be appropriate.
-
Requires private health insurers to pay health care providers for COVID-19 testing either on the basis of a contracted rate or the rate that the provider publishes on its website. This provision is intended to avoid "surprise bills" caused by health care providers charging to individuals the portion of billed price not covered by an insurer.
-
Requires private health insurers to cover, with no cost sharing, future COVID-19 vaccines and other preventive services that prevent or mitigate COVID-19 soon after they are developed. (The CARES Act also eliminates cost sharing for future COVID-19 vaccines in Medicare.)
Paycheck Protection Program and Health Care Enhancement Act (COVID Phase 3.5)
The President signed H.R. 266, the Paycheck Protection Program and Health Care Enhancement Act, into law on April 24, appropriating $484 billion for various COVID-19 relief purposes, including funding for hospitals and other health care providers and COVID-19 testing.
Provides Additional $75 Billion Nationwide in Relief Funding for Hospitals and Other Health Care Providers. The Paycheck Protection Program and Health Care Enhancement Act (which we henceforth refer to as COVID Phase 3.5) provides an additional $75 billion nationwide to the PRF—on top of the $100 billion provided through the CARES Act—to assist hospitals and other health care providers with covering expenses and lost revenue due to COVID-19. COVID Phase 3.5 does not prescribe how the federal government must allocate this new funding from PRF. Accordingly, the portion of this new funding that will be provided to California hospitals and health care providers is unknown. However, we note that initial rounds of funding from PRF have been made and that the federal government has set some priorities for allocating further rounds of funding (described earlier in this post under our discussion of the CARES Act). It is possible that this new funding from PRF will be allocated according to similar priorities.
Provides $25 Billion Nationwide for COVID-19 Testing-Related Activities. COVID Phase 3.5 provides an additional $25 billion to PHSSEF available nationwide for COVID-19 testing-related activities. (We discuss previous funding provided to PHSSEF earlier in this post under our discussion of the CARES Act.) In addition, COVID Phase 3.5 requires each state, locality, territory, or tribal organization receiving testing funds to submit a strategic testing plan to DHHS. This funding may be used for a variety of purposes, such as researching, developing, or purchasing tests (including antibody tests), securing or renovating facilities to improve testing infrastructure and production capacity, purchasing supplies and equipment (including PPE), conducting surveillance and epidemiology, scaling up testing, or developing the workforce. Any products purchased with these funds can be deposited in the Strategic National Stockpile (discussed earlier in this post under our discussion of the CARES Act). This funding is allocated as follows:
-
At Least $11 Billion Nationwide for Public Health Activities. The federal government is providing at least $11 billion nationwide in grants to state and local governments, territories, and tribal organizations, as follows:
DHHS has provided $10.25 billion to states through CDC’s existing Epidemiology and Laboratory Capacity for Prevention and Control of Emerging Infectious Diseases cooperative agreement. Funding will support development, purchase, administration, processing, and analysis of COVID-19 tests, surveillance, contact tracing, and other related activities. California has received $499.2 million, while Los Angeles County has received $289 million. This brings total CDC funding for California (including Los Angeles County) up to $941 million, as follows in Figure 1 below.
DHHS is providing $750 million to tribes, tribal organizations, and urban Indian organizations through the Indian Health Service. The specific amount that will be allocated within California is currently unknown.
-
$825 Million Nationwide for Health Centers and Rural Health Clinics. The federal government will provide $825 million in total nationwide grants to health centers and rural health clinics, allocated as follows:
$600 million has been distributed nationwide to health centers (as defined in the Public Health Service Act) and Federally Qualified Health Centers. About $97 million of this distribution went to health centers and Federally Qualified Health Centers in California.
$225 million will be distributed nationwide to rural health clinics. So far, $13.1 million of this amount has been distributed to California rural health clinics.
-
Up to $1 Billion Nationwide for COVID-19 Testing for the Uninsured. Up to $1 billion will be distributed nationwide for COVID-19 testing for the uninsured (as defined under FFCRA). The amount of this funding that would be allocated to California is unknown.
-
Other Funding for COVID-19 Testing-Related Activities Will Support National Efforts. COVID Phase 3.5 also provides funding for COVID-19 testing-related activities that would support national efforts, benefits of which would accrue to California. This includes (1) at least $1.8 billion to the National Institutes of Health, (2) at least $1 billion to the CDC, (3) no less than $1 billion to the Biomedical Advanced Research and Development Authority, and (4) $22 million to the Food and Drug Administration.
Figure 1
Total Funding to California Through the Centers for Disease Control and Prevention
(In Millions)
|
CPRSAA/Transfers |
CARES Act |
COVID Phase 3.5 |
Total |
|
|
State of California |
$63.6 |
$41.9 |
$499.2 |
$604.4 |
|
Los Angeles County |
27.4 |
20.2 |
289.0 |
336.6 |
|
Totals to California |
$91.0 |
$62.1 |
$788.2 |
$941.0 |
|
CPRSAA = Coronavirus Preparedness and Response Supplemental Appropriations Act; CARES Act = Coronavirus Aid, Relief, and Economic Security Act; and COVID Phase 3.5 = refers to the Paycheck Protection Program and Health Care Enhancement Act. |
||||