LAO Contact

July 13, 2023
Mental Health Services Act
Proposed Restructuring of the MHSA Funding Categories and Impacts on County Spending
Summary. This post is one of a series of Legislative Analyst’s Office posts on the various components of the Governor’s Behavioral Health Modernization proposal, reflected in SB 326 (Eggman), as amended on June 19, 2023. The Mental Health Services Act (MHSA) allocates funding primarily to counties to provide mental health services and establishes broad categories for how counties can spend the funding. The Governor’s proposal would change the funding categories under the MHSA, requiring counties to allocate more MHSA funding towards Full-Service Partnerships (FSPs) and housing interventions. We find that the Governor’s proposal would reduce overall county discretion and likely result in counties spending less on a number of current programs. We find that the administration’s justification of its proposed changes is incomplete and we provide several questions for the Legislature to ask the administration to assess whether the proposal is warranted. For example, can the administration provide evidence that the proposal is likely to result in better behavioral health outcomes for the population as a whole? What are the trade-offs in reducing county spending flexibility?
Background
Current MHSA Funding Categories
Funding Categories and Allocation of MHSA Revenues Under Current Law. Approved by voters in 2004, the MHSA places a 1 percent tax on personal income over $1 million and dedicates the associated revenues to mental health services. The vast majority of MHSA revenues—at least 95 percent—goes directly to counties, which use it to support a variety of services for individuals with or at risk of mental illness. The MHSA establishes broad categories for how counties can spend the funding, including the percent of funds which must—or sometimes may—be spent on specific kinds of activities. Figure 1 provides a high-level summary of the current three broad spending categories, along with examples of the types of services/activities funded under them and the percentage of MHSA revenues allocated to them.
Figure 1
Allocation of Current MHSA Funding Categories
|
Current MHSA Funding Category |
Examples of Types of Services/Activities |
MHSA Revenue Allocation |
|
Community Services and Supports |
|
76 percent |
|
Prevention and Early Intervention |
|
19 percent |
|
Innovation Programs |
|
5 percent |
|
MHSA = Mental Health Services Act. |
||
Largest Funding Category by Far—Community Services and Supports (CSS)—Affords Counties Significant Discretion. As shown in Figure 1, 76 percent of MHSA county funding must be spent on CSS, which supports a broad range of direct service provision (such as outpatient treatment). In addition, about 20 percent of CSS funding can be used for capital facilities, technological needs, workforce, education and training, and deposits for counties’ prudent reserves. While not required by MHSA, state regulations currently require counties to use 50 percent of CSS funding for FSPs. FSPs provide mental health and wraparound services—such as housing and employment support—for individuals with the greatest mental health needs. As also shown in the figure, 19 percent of MHSA funding for counties must be used on Prevention and Early Intervention (PEI) activities, which are aimed at preventing mental illnesses before they become severe. The remaining county funding (5 percent) is directed to innovation programs, with the goal of encouraging counties to experiment with new approaches to treating and preventing mental illness.
Governor’s Proposal
Funding Categories
Funding Categories and Allocation of MHSA Revenues Under Governor’s Proposal. The Governor’s proposal makes major changes to how counties allocate MHSA revenues beginning July 1, 2026. The majority of MHSA funding—92 percent—still would go to counties, but the proposal shifts the focus of the funding allocations towards both FSPs (as a statutory requirement) and housing. Figure 2 provides a high-level summary of the four proposed categories for county funding, along with examples of the types of services/activities funded under them and the percentage of MHSA revenues allocated to them.
Figure 2
Allocation of Proposed MHSA Funding Categories
|
Proposed MHSA Funding Category |
Examples of Types of Services/Activities |
MHSA Revenue Allocation |
|
Full‑Service Partnershipsa |
|
35 percent |
|
Housing Interventions |
|
30 percent |
|
50 percent must be for individuals who are chronically homelessness. |
||
|
Behavioral Health Services and Supports |
|
30 percent |
|
Majority must be for early intervention. |
||
|
Population‑Based Mental Health Substance Use Disorder Prevention |
|
5 percent |
|
Population‑based prevention programs cannot include the provision of services to individuals. |
||
|
aUnder the proposal, housing services provided to Full‑Service Partnership participants would be counted under the Housing Intervention category. |
||
|
MHSA = Mental Health Services Act. |
||
Proposal Increases Spending on FSPs and Housing. The Governor’s proposal would make FSP spending a statutory requirement for counties. Specifically, counties would be required to spend 35 percent of funding on FSP programs. In addition, under the Governor’s proposal, 30 percent of MHSA county funding would be used on housing intervention programs for the provision of housing or infrastructure funding to create new housing. Housing intervention services provided to FSP participants would be counted under this category. Examples of eligible programs include rental and operating subsidies, family housing, and the nonfederal share of Medi-Cal-eligible transitional rent. The proposal also requires that 50 percent of the funds in this category be used on housing interventions for individuals who are chronically homeless.
Proposal Decreases Flexible Spending. The funding category under the Governor’s proposal that affords the most spending discretion to counties—Behavioral Health Services and Supports (BHSS)—is significantly smaller than the similar category under current law (CSS). This funding category—30 percent of MHSA county funding—would be used for services and supports for adults, older adults, and children that are not provided under FSPs; early intervention programs (a majority of the funding); innovative behavioral health pilots and projects; capital facilities; technological needs; workforce; education and training; and deposits for counties’ prudent reserves.
Assessment
Methodology and Data Limitations
Data Limitations in Assessing Counties’ Current Spending. To assess the impacts of the proposal on county spending, we collected 2021-22 program expenditure data from 50 counties (reflecting nearly 99 percent of California’s population). Below, we outline the data limitations that prevent us from precisely measuring (1) the extent to which current spending aligns with the proposed new funding categories and the associated spending targets/limits and thus (2) how county spending could change under the Governor’s proposal. Despite these limitations, however, our estimate still provides a baseline for evaluating how current expenditures may align with the proposed categories.
As data are reported individually by each county, we are required to make assumptions about the nature of services provided under programs, the titles of which can vary county by county.
Information on what current programs include housing interventions are not captured explicitly in current reporting. To create our estimate, we used program names across counties to determine if they might qualify as housing interventions. This evaluation criteria may over or underestimate the current spending that would qualify under the Housing Interventions category in the Governor’s proposal.
We are unable to estimate the current program expenditures that would qualify under the Population-Based Mental Health Substance Use Disorder Prevention category. Based on the currently available data, there is no way to determine which programs would be classified as population-based prevention programs rather than prevention programs serving individuals.
Our analysis includes the most current, publicly available, annual expenditure data. There may be changes in the types of programs and services funded on a year-to-year basis that are not captured in our analysis and 2021-22 data may not be representative of counties’ funding priorities over time.
We calculated and classified program expenditure data as statewide totals. There are differences among counties in both how expenditures are allocated within current categories and how expenditures are likely to align with the proposed categories. We discuss the importance of understanding these county-level differences later in this post.
The creation of new funding categories and spending targets/limits under the Governor’s proposal would create different incentives and priorities for counties. While we estimate the extent to which current county spending aligns with the proposed funding categories and spending targets/limits, how counties may shift program expenditures if the proposal passes is unknown.
Comparing County Spending Categories
Significant Level of Discretion Afforded to Counties Within Current Funding Categories. The left side of Figure 3 displays counties’ 2021-22 program expenditures (totaling $2.1 billion) by funding category as well as examples of the programs that fall under current MHSA categories as reported in the 2021-22 expenditure data. The data reflect that while there are a few requirements within the CSS, PEI, and Innovation categories, counties are able to fund a wide variety of programs to meet local needs. For example, while at least half of CSS funding must be used on FSPs, counties can spend the remaining available funds on crisis intervention, outpatient services, wellness centers, or various capacity building projects like technological needs. Similarly, PEI can be used for a wide variety of prevention and early intervention services such as school-based support services or outreach to vulnerable populations.
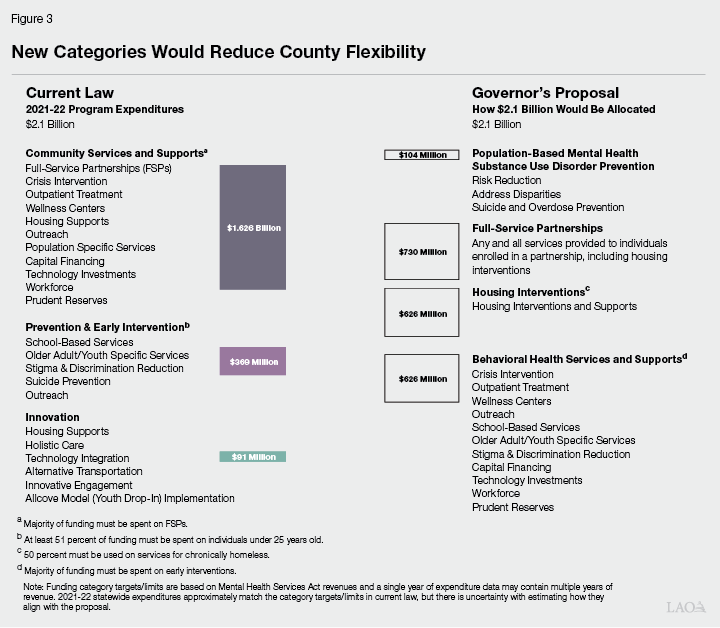
Governor’s Proposal Reduces Overall County Discretion by Focusing Funding on FSPs and Housing Interventions. The right side of Figure 3 shows how a total expenditure amount of $2.1 billion (the 2021-22 total) would be broadly allocated under the Governor’s proposed funding categories and spending targets/limits. As shown, the Governor’s proposal creates a category for FSPs (where before they were a subcategory within CSS) as well as housing interventions. While counties have some discretion in how to focus funding within these two new categories, the proposal is fairly prescriptive in the types of programs within these categories eligible for MHSA funding. As a result, a large portion of programs currently funded across the CSS, PEI, and Innovation categories would only be eligible to be funded through the newly created BHSS category under the Governor’s proposal. While the current categories have some restrictions on what programs may be funded, they are broad enough to give counties flexibility to direct funds to certain services based on local determinations. However, under the proposal, counties have a smaller share of MHSA revenue available for flexible spending on programs.
Possible Changes to County Spending
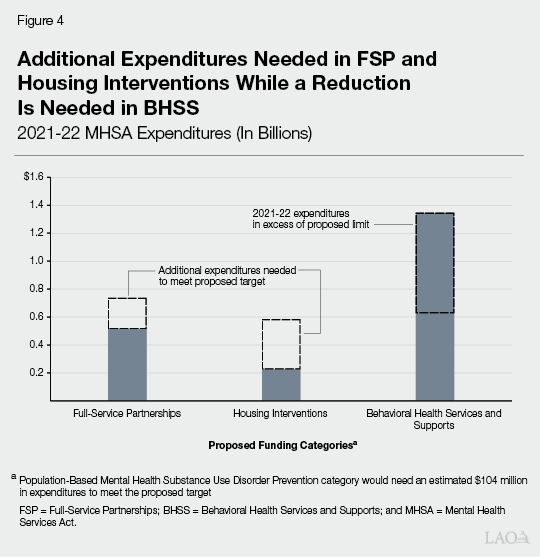
New Funding Categories Likely Would Require Counties to Spend More on Certain Programs, Less on Others. Figure 4 shows how we estimate current program expenditure levels would align with the proposed categories. Based on current expenditures, counties would need to increase spending on FSP and Housing Intervention, substantially so in the case of Housing Interventions. We estimate that relative to 2021-22 program expenditures for FSP ($515 million) and Housing Interventions ($226 million), counties would need to increase spending by $121 million and $493 million, respectively, to reach the proposed funding targets. Conversely, counties would need to redirect or reduce expenditures on programs that fall under the proposed BHSS category limit. Whereas current expenditures that would be eligible under the BHSS category currently make up around 60 percent of MHSA dollars, under the proposal, this category would be capped at 30 percent. Consequently, these expenditures would need to be reduced from $1.34 billion to $621 million.
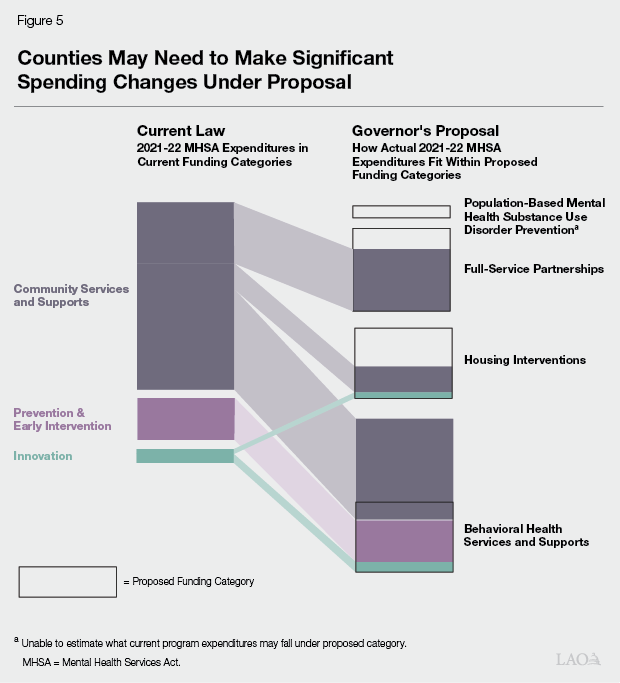
Current Programs That Would Fit Under the Proposed BHSS Category Likely Would Be Reduced Due to Funding Limits. Figure 5 provides a breakout of how current funding categories appear to align with the Governor’s proposed categories. As shown in the figure, linking the current funding categories to the proposed ones, we assume that programs currently under the CSS category would be classified under the FSP, Housing Interventions, and BHSS categories. We assume that all PEI programs would fall under the BHSS category, while Innovation programs would fall under Housing Interventions and BHSS. A number of current CSS and PEI programs, that make up the majority of current spending that would fit within the new BHSS category, would likely see reductions in MHSA funding. This is compounded by the fact that the majority of BHSS funds must be spent on early intervention programs, further limiting what current expenditures can align with the proposed funding category limit for BHSS programs. Based on how counties reported program information, counties may need to reduce funding for outpatient services, crisis response, prevention services, and outreach.
Issues for Legislative Consideration
Administration’s Justification of Proposed Changes Incomplete. The administration’s proposal reduces county flexibility and shifts the focus of MHSA funding to FSPs, housing interventions, and early intervention programs. This change would reduce funding available for several current programs funded through the MHSA. Under the proposal, counties would need to increase MHSA expenditures on FSPs and housing interventions, while potentially reducing outpatient services, crisis response, prevention services, and outreach. The administration has not provided an assessment of how the changes may negatively impact current services. For example, while the administration cites the shortfall in psychiatric treatment beds as a primary justification for the focus on housing interventions, the administration has not provided the rationale for using MHSA—given the trade-offs—to address this and other issues. Consequently, as the Legislature considers the proposal, we recommend asking the administration certain questions to assess whether the proposal is warranted. The rest of this section outlines our recommended questions.
Would Statewide Behavioral Health Outcomes Be Improved by Shifting Funding Focus? The proposal would increase spending on FSPs and housing significantly. The Legislature has noted that individuals receiving FSP services experienced a 68 percent decline in homelessness in one study. Additionally, the administration cites the linkage between safe and affordable housing with successfully treating serious mental illness and substance use disorder research, including research that identified a shortage of psychiatric beds in California. While research supports the administration’s proposed interventions to improve outcomes for individuals experiencing or at risk of homelessness, MHSA services benefit a broader population of Californians. Consequently, some beneficiaries of MHSA may no longer receive certain services under the proposal. On net, can the administration provide evidence that the proposal is likely to result in better behavioral health outcomes for the population as a whole? Why does the administration propose using the MHSA as opposed to other funds to support the priorities reflected in the proposal?
What Are the Trade-Offs in Reducing County Spending Flexibility? The administration’s proposed funding categories would reduce the amount of overall flexibility afforded counties in two ways: (1) by creating only one category, BHSS, with just 30 percent of MHSA funding that can accommodate flexible program expenditures and (2) by including a wide variety of programs that counties would need to spend funds on in BHSS (early intervention, capital facilities, deposits into prudent reserves, among others) that would reduce funding available for other county initiatives. In effect, the proposal would shift the discretion in setting MHSA funding priorities away from counties to the administration. This potentially deprives the state of county-level expertise in program implementation and understanding the needs of its residents. The Legislature may wish to ask the administration, along with counties, about the trade-offs of reducing county flexibility in MHSA spending. Additionally, the Legislature should consider whether the shift towards a top-down approach in the use of MHSA funds aligns with the Legislature’s vision of the program.
How Does the Proposal Complement Recent Initiatives to Serve Individuals Experiencing Homelessness and Behavioral Health Conditions? The proposed Housing Interventions category includes a requirement that the majority of funding be for services to individuals who are chronically homeless. The administration has not yet sufficiently articulated how its proposal complements a recent major initiative approved by the Legislature—the Behavioral Health Bridge Housing Program—to provide housing supports to homeless individuals with behavioral health conditions.
What Are the Impacts on Individual Counties? Our analysis evaluates how the shift in funding categories could impact county expenditures at the statewide level. However, as noted, the actual impact to individual counties could vary. The Legislature could ask the administration, along with counties, for information on the anticipated distributional impacts of the proposal on a county-by-county basis. This information would give the Legislature a more comprehensive picture of local impacts.