Juwan Trotter

March 6, 2025
The 2025-26 Budget
In-Home Supportive Services
Summary
For the In-Home Supportive Services (IHSS) program, the Governor’s 2025-26 budget proposes approximately $10.6 billion General Fund, an increase of $1.1 billion (11 percent) from the Governor’s revised 2024-25 budget estimate. This increase would bring total program funding to $28.5 billion total funds in 2025-26 (an increase of $2.6 billion—10 percent—compared to revised estimates for 2024-25). The primary drivers of this year-to-year General Fund cost increase include continued estimated growth in two of the three primary IHSS cost drivers—caseload (7 percent) and cost per hour (2.9 percent). The average monthly hours per case are estimated to remain flat year-over-year. While the administration does not include any major new IHSS related proposals as part of the Governor’s 2025-26 budget, throughout this post, we provide updates on some of the most recent, prior-year policy changes. Finally, while the proposed budget initially appears reasonable, we do flag some outstanding questions we have about some potential cost pressures we will be monitoring.
Background
Overview of the IHSS Program. The IHSS program provides personal care and domestic services to low-income individuals to help them remain safely in their own homes and communities. In order to qualify for IHSS, a recipient must be aged, blind, or disabled, and in most cases have income below the level necessary to qualify for the Supplemental Security Income/State Supplementary Payment cash assistance program (for example, about $1,207 a month for an aged and/or disabled individual living independently in 2024-25). IHSS recipients generally are eligible to receive up to 283 hours per month of assistance with tasks such as bathing, dressing, housework, and meal preparation. Social workers employed by county welfare departments conduct an in-home assessment of an individual’s needs in order to determine the amount and type of service hours to be provided. In most cases, the recipient is responsible for hiring and supervising a paid IHSS provider—oftentimes a family member or relative. The average number of service hours that will be provided to an estimated 771,650 IHSS recipients is projected to be 123.7 hours per month in 2025-26 (which is the same number of hours per case estimated for 2024-25).
IHSS Costs Split Between Federal Government, State, and Counties. IHSS costs are shared by the federal government, state, and counties. Since IHSS primarily is delivered as a Medi-Cal benefit, the federal share of cost is determined by the Medicaid reimbursement rate, which typically is 50 percent. The state receives an enhanced federal reimbursement rate for many IHSS recipients who receive services as a result of the Patient Protection and Affordable Care Act expansion (90 percent federal reimbursement rate) and the Community First Choice Option waiver (56 percent federal reimbursement rate). Overall, the effective federal reimbursement rate for IHSS is about 54 percent. The remaining nonfederal share of IHSS costs is covered by the state and counties. Historically, counties paid 35 percent of the nonfederal share of IHSS service costs and 30 percent of the nonfederal share of IHSS administrative costs. Beginning in 2012-13, however, the historical county share-of-cost model was replaced with an IHSS county maintenance-of-effort (MOE), meaning county costs reflect a set amount of nonfederal IHSS costs (that may be adjusted annually by a growth factor and a portion of locally negotiated wage increases) as opposed to a certain percent of nonfederal IHSS costs. The state is responsible for covering the remaining nonfederal share of costs not covered by the IHSS county MOE.
Budget Overview and Assessment: Caseload, Cost Per Hour, and Hours Per Case Update
Caseloads Are Growing at an Increasing Rate… Figure 1 shows the growth rate and key policy changes in IHSS since 2014-15. (Subsequent sections of this post discuss the impacts of these policy changes.) As shown in the figure, the growth rate declined steadily from 2016-17 through 2020-21. Despite this declining growth rate, the caseload continued to grow during this period. The caseload then began to grow at a faster rate over the following years, reaching a growth rate of 7.1 percent in 2023-24. The Governor’s 2025-26 budget assumes the caseload will continue growing at this faster rate, estimating a growth rate of 7.5 percent in both 2024-25 and 2025-26.
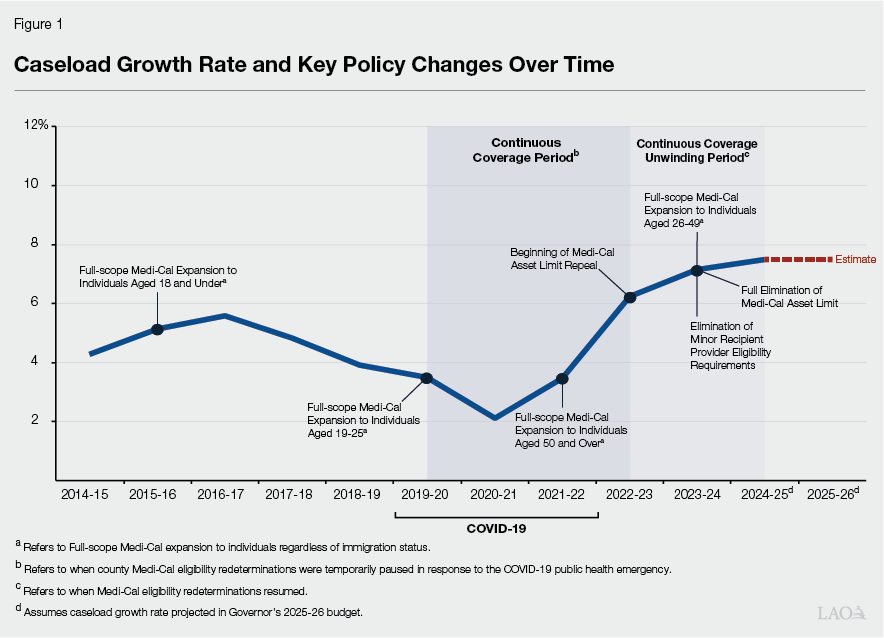
…However, Caseload Growth Rates Have Historically Been Variable. Although the IHSS caseload has grown at a positive rate for all but two years since 1991-92 (our first year of readily available data), the rate of that growth has been variable. In 1991-92, the caseload grew at a rate of 8.1 percent. The following year (1992-93), the caseload growth dropped to 1.4 percent. Over the next eight years, growth rates fluctuated between 3 percent and 8 percent, until reaching a peak growth rate of 10.2 percent and 10.4 percent in 2001-02 and 2002-03, respectively. Caseload growth then hovered between 4.5 percent and 8 percent for the next six years. However, following the passage of several service reductions, eligibility changes, and anti-fraud initiatives, the IHSS caseload actually declined year-over-year by 0.2 percent in 2009-10 and declined again by 0.02 percent in 2011-12.
Legislative Analyst’s Office (LAO) Caseload Assessment. The IHSS caseload, along with the cost per hour, is a key IHSS cost driver and can be influenced by several factors—including demographic changes, as well as federal and state policy decisions. Based on the most recent actual caseload data, it appears that the IHSS caseload is growing at a faster rate than assumed in the Governor’s 2025-26 budget proposal. This leads us to believe that projected IHSS costs may ultimately be higher than what is captured in the Governor’s budget for both 2024-25 and 2025-26. As such, we will continue to monitor caseload growth over the coming months and continue working to better understand the caseload impacts of various policy choices, including the recent Medi-Cal eligibility expansions and asset limit elimination (we provide more detailed information on both eligibility changes below).
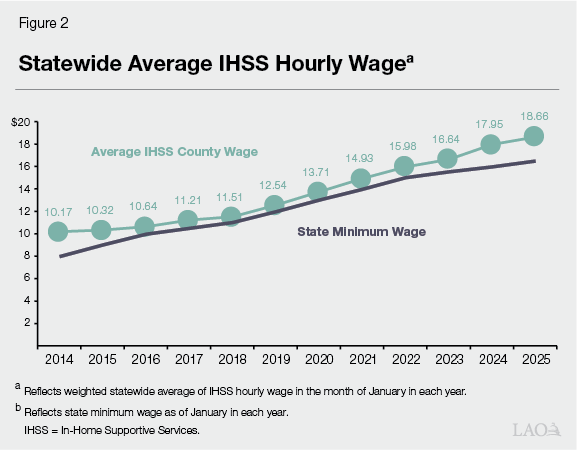
Cost Per Hour Continues to Increase. The Governor’s budget estimates that the cost per hour of IHSS services will increase from $21.03 in 2024-25 to $21.65 in 2025-26. The majority of the cost per hour is associated with IHSS wages (estimated to be an average of $18.66 per hour as of January 2025), but also includes other provider benefits and administrative costs. As shown in Figure 2, the average IHSS hourly wage has increased by 5.7 percent annually since 2014. The growth in IHSS hourly wages in part is due to increases to the state minimum wage—from $8 per hour in January 1, 2014 to $16.50 per hour in January 1, 2025. Pursuant to current law, the state minimum wage will continue to increase by inflation annually. Additionally, counties may establish IHSS hourly wages above the state minimum wage through local wage ordinances or, more commonly, collectively bargained agreements. The state, federal government, and counties share the cost of IHSS wages.
Hours Per Case Estimated to Remain Flat Despite Consistent Growth in Recent Years. The Governor’s budget estimates that average monthly hours per case will remain flat at 123.7 hours in both 2024-25 and 2025-26. However, historically, average hours per case have consistently increased year-over-year. For example, between 2017-18 and 2023-24, average hours per case increased from about 108 hours per month to just over 122 hours per month. This was an average annual increase of about 2 percent. We are working with the administration to better understand the reason for assuming the average hours per case will not increase in the budget year. This is important because an increase in average hours per case in 2025-26 could result in a General Fund cost pressure that is not currently captured in the Governor’s budget proposal
Update on Full-Scope Medi-Cal Expansion to Individuals Regardless of Immigration Status
Historically, income-eligible undocumented individuals only qualified for “restricted-scope” Medi-Cal coverage, which covers their emergency- and pregnancy-related service costs. In general, beneficiaries of restricted scope Medi-Cal were not eligible for IHSS. The state has expanded comprehensive, or “full-scope,” Medi-Cal coverage, including IHSS eligibility, to all income-eligible children (effective May 2016), income eligible adults aged 19-25 (effective January 2020), income eligible older adults aged 50 and over (effective May 2022), and income eligible adults aged 26-49 (effective January 2024)—effectively covering all income-eligible individuals regardless of their immigration status.
Costs Revised Downward for Recipients Age 26-49. As shown in Figure 3, for the 26 to 49 expansion age group, the Governor’s budget includes roughly $3.4 million General Fund in 2024-25. This is approximately $17.8 million less than what was originally appropriated in the 2024-25 budget. The administration notes that this revised cost estimate reflects the administration’s use of an updated methodology which utilizes actual paid caseload data rather than caseload projections from the Department of Health Care Services.
Figure 3
Evolution of Caseload and Service Cost Estimates for
Full‑Scope Medi‑Cal Expansion to Individuals
Regardless of Immigration Status
(General Fund, In Millions)
|
Expansion Group |
2024‑25 |
2024‑25 |
2025‑26 |
|
18 and Under |
|||
|
Cost |
$1.5 |
$2.7 |
$2.8 |
|
Average Monthly Caseload |
49 |
88 |
88 |
|
19 ‑ 25 |
|||
|
Cost |
$1.6 |
$2.0 |
$2.9 |
|
Average Monthly Caseload |
60 |
75 |
107 |
|
26 ‑ 49 |
|||
|
Cost |
$21.2 |
$3.4 |
$5.4 |
|
Average Monthly Caseload |
785 |
125 |
195 |
|
50 and Above |
|||
|
Cost |
$66.9 |
$72.3 |
$106.1 |
|
Average Monthly Caseload |
2,476 |
2,660 |
3,859 |
|
Totals |
|||
|
Cost |
$91.2 |
$80.4 |
$117.2 |
|
Average Monthly Caseload |
3,370 |
2,948 |
4,249 |
Majority of Overall Expansion Group Caseload and Costs Continues to be Associated With 50 and Over Expansion. As shown in Figure 3, the majority of the caseload and cost increases associated with the Medi-Cal expansion to individuals regardless of immigration status, is attributable to the 50 and above age group. For 2024-25, the Governor’s revised budget includes roughly $72 million General Fund. This is approximately $5.4 million more than what was originally appropriated in the 2024-25 budget. This is then expected to increase in 2025-26 with the Governor’s proposed budget including roughly $106 million General Fund for this group.
Utilization Rates for Expansion Population Lag Behind Overall Population. Available IHSS case information provides the percent of authorized IHSS cases that receive services. We call this the IHSS utilization rate. Historically, The IHSS utilization rate has been quite high—in the high-80 percent to low-90 percent range. Utilization rates for the most recent expansion groups—the 26-49 and 50 and above age groups (currently, there is no readily available utilization rate data for the age 18 and under or age 19-25 expansion groups)—have lagged behind these historical utilization rates. In the most recent months of available data (January 2024 to June 2024), the 26-49 expansion age group has had an average utilization rate of 59 percent, while the 50 and above expansion age group has experienced an average utilization rate of 70 percent. Although the utilization rate for the 50 and above expansion age group is lower than the utilization rate for the overall population, it has been increasing over time. The administration has noted that because undocumented individuals remain ineligible to be IHSS providers, and a majority of IHSS recipients receive services from a family member, recipients with undocumented family members may have a more difficult time securing an eligible provider. Additionally, since these are new expansions, it may take time for recipients and providers to fully become aware and utilize the new benefit.
Update on Provider Eligibility for Minor Recipients
Elimination of Minor Recipient Provider Eligibility Requirements Expands IHSS Access. Historically, a parent could only become the paid IHSS provider for their minor child if the care needs of their child would prevent the parent from maintaining full-time employment. If the care needs of the child did not prevent the parent from maintaining full-time work, a provider other than the parent could be hired. It is our understanding from the department that this requirement particularly impacted minor recipients with parents who were undocumented. In these cases, parents were deemed unable to work due to their immigration status, not due to the needs of the child, and this resulted in children of these parents being unable to secure anyone, including their parents, to provide authorized IHSS services. By eliminating the minor recipient provider eligibility requirements, IHSS-eligible minor recipients are now treated like all other IHSS recipients when it comes to the selection of a provider. As of December 2024, roughly 91 percent of minor recipients had a paid provider—which is slightly higher, but close to, the utilization rate for the overall IHSS population. The Governor’s budget includes roughly $47 million in 2024-25 and $49 million in 2025-26, for support of this policy change. We will continue to work with the administration to better understand estimated expenditures for this policy change and will provide updates at May Revision if necessary.
Update on Medi-Cal Asset Limit Repeal Implementation
Phasing in Medi-Cal Asset Limit Repeal Has Increased IHSS Caseload. Historically, low-income seniors and persons with disabilities had to have assets at or below $2,000 (or $3,000 for couples) to be eligible for Medi-Cal. The 2021-22 budget included legislation to fully phase out the asset limit in Medi-Cal. To this end, the asset limit was first raised from $2,000 to $130,000 for individuals and from $3,000 to $195,000 for couples in July 2022. The asset limit was subsequently fully eliminated January 1, 2024. The complete removal of the asset limit results in more seniors and persons with disabilities becoming eligible for Medi-Cal services, including IHSS. The Governor’s proposed budget includes about $23.5 million General Fund in 2024-25 to provide services to the estimated 1,900 seniors and persons with disabilities who will become eligible for Medi-Cal and also enroll in IHSS as a result of this policy change. This represents a decrease of approximately $24 million from the 2024-25 Budget Act estimates. This decline represents a decrease in projected caseloads. Additionally, going forward, the administration has noted that they will be including estimates for this population in the basic services trend estimate. In previous years, the administration has noted that they currently do not have a methodology in place to be able to track how many actual IHSS recipients enter the program as a result of this asset limit change. However, we believe that the asset limit repeal—along with other noted Medi-Cal expansions—are contributing factors to this caseload growth.
Update on Permanent Backup Provider System
Permanent Backup Provider System Established in 2022-23 Budget. The 2021-22 budget included $5 million General Fund to create a permanent IHSS backup provider system on January 1, 2022, contingent on a policy framework being adopted in statute. However, a policy framework for the permanent backup provider system was not adopted within the 2021-22 budget period, resulting in the initial $5 million allocation going unspent. The 2022-23 budget codified a policy framework for the permanent backup provide system. Under the permanent backup provider system, a recipient whose regular provider is not available, but who has an urgent need or whose health and safety will be at risk without a backup provider, can receive up to 80 hours (if recipient is non-severely impaired) or 160 hours (if recipient is severely impaired) of backup provider services per fiscal year. Additionally, backup providers are paid $2 above the local IHSS hourly wage rate.
Backup Provider System Has Been Rightsized Over Time. The 2023-24 Budget Act appropriated approximately $15.7 million General Fund for Backup Provider services. The 2024-25 Budget Act reduced the appropriation to approximately $5.6 million General Fund based on updated estimates of use. The Governor’s updated estimates for 2024-25 now forecast Backup Provider service costs to be roughly $420,000 General Fund. Though expenditures for the Backup Provider system have grown over time, the ramp up for this program has continued to remain below expectations. Since the program began in October 2022 through June 2024 (the most recent month of expenditures data), less than $900,000 total funds have been spent on Backup Provider services. At this time, we do not have any concerns with the administration’s estimates. We will continue to monitor updated expenditure levels and provide updates in the May Revision if necessary.
Update on Paid Sick Leave Implementation
Paid Sick Leave (PSL) Established for IHSS Providers in 2018-19. PSL became available on July 1, 2018 for IHSS providers who worked a certain number of hours within a calendar year. In 2018-19, the maximum amount of PSL an IHSS provider could accrue was eight hours per year. This increased to 16 hours in 2020-21, 24 hours in 2022-23, and 40 hours on July 1, 2024. The Governor’s proposed budget includes roughly $89 million in 2024-25 and $122.3 million in 2025-26 for PSL. We will continue to work with the administration to monitor the utilization of paid sick leave hours. However, based on our review of our most recent paid sick leave data, we believe that this estimate appears reasonable.
Issues for Legislative Consideration
Career Pathways Expenditure Update. Under the American Rescue Plan Act of 2021, the federal government made available additional funding to be used toward Medicaid-funded Home and Community Based Services (HCBS) and programs. A portion of these funds were allocated for the development and implementation of the IHSS Career Pathways program, designed to provide specialized training opportunities and financial bonuses for IHSS providers (Please see our analysis of the Governor’s 2024-25 Budget for more information).
On September 16, 2024, the Department of Social Services (DSS) ended training enrollment for the IHSS Career Pathways program, ahead of schedule. This was done because projected expenditures at that time had already surpassed the programs HCBS allocated funds. Providers who had already completed trainings were still able to claim incentive payments up to November 2024. As of December 2024, the Career Pathways program had accrued nearly $90 million worth of expenditures above their HCBS allocation. This was then offset by roughly $30 million in increased HCBS Funds. This leaves, as of December 2024, a funding gap of at least $60 million. The Joint Legislative Budget Committee has requested the administration to provide a final reconciliation of the total funding gap, as well as, a plan to fully address program overages by April 1, 2025, or 30 days after the reconciliation is complete—whichever comes first.
Collective Bargaining Analysis Update. The 2023-24 Budget Act provided DSS with $1.5 million to analyze the costs and benefits of transitioning the IHSS program from the current county level collective bargaining model to a statewide or regional collective bargaining model. Among other issues, this analysis was requested to include a fiscal analysis of the cost of making such a transition, including potential fund sources and potential impacts on the current realignment structure. Additionally, this analysis was to discuss how this transition may impact workforce recruitment and retention. Though this analysis was required to be released no later than January 2025, DSS has communicated that they are in the final processes of releasing their analysis. We will be reviewing this report when it becomes available.
Administrative Funding Rebase Efforts. The Department of Social Services was required in statute (Chapter 46 of 2024 [AB 161, Committee on Budget]) to review the budgetary methodology used to determine annual funding for the county administration of IHSS alongside workload and administrative costs. This review was required to begin with fiscal year 2025-26 and every three years thereafter. It is our understanding that this work is currently underway. The administration is also required to provide information to the appropriate budget committees on the review and how it may impact costs. The Legislature may wish to ask the administration when it expects this information will be available.