Ryan Woolsey

March 5, 2026
The 2026-27 Budget
County Administration and H.R. 1 Implementation
Summary
H.R. 1 Notably Impacts Medi‑Cal and CalFresh Eligibility Administration. Medi‑Cal and CalFresh are overseen by the state but are administered locally by counties, with a focus on eligibility determination. H.R. 1 makes major changes to Medi‑Cal and CalFresh that largely will result in lower enrollment in the programs. One significant area of change under H.R. 1 is the expansion and creation of community engagement requirements (generally, work requirements). These new requirements—along with other changes—have significant impacts for counties’ administration of the programs.
Governor’s Budget Proposes Some Adjustments Related to H.R. 1 Implementation. In Medi‑Cal, the Governor’s budget maintains the existing level of funding for county administration, making no adjustments to account for H.R. 1 implementation. The administration has indicated that it is working with counties to better understand H.R. 1 impacts on Medi‑Cal administration so that county administrative funding can be revisited at the May Revision. In CalFresh, the Governor’s budget reflects the higher state and county share of costs imposed by H.R. 1 and provides some additional funding for counties to implement expanded work requirements, but this is more than offset by funding reductions tied to anticipated disenrollment.
Counties Are Key to Addressing Error Rates… The state faces significant increased CalFresh costs related to payment error rates as early as October 2027. Potential future financial penalties related to Medi‑Cal payment errors are less certain and would not take effect until October 2029 at the earliest but could be significant. County implementation of H.R. 1 and efforts to reduce payment error rates will be affected by state policy, but also by strategies and resource allocation in individual counties. We recommend that the Legislature direct the administration and counties to report on what are the major drivers of payment error rates and plans to manage them.
…And Avoiding Disenrollment Due to Administrative Burden. Automating verification processes and relying on all available data sources is a key strategy to mitigate the risk of disenrollment due to administrative burden. The Legislature could consider the trade‑offs of providing additional funding for county administration to allow counties to spend more time carefully working with enrollees to further limit disenrollment. If additional funding is provided, we recommend that the augmentation be temporary until the level of ongoing workload related to H.R. 1 is better understood.
Baseline Medi‑Cal Administration Budgeting Approach Has Shortcomings. The current approach to budgeting Medi‑Cal county administration funding lacks a clear link to workload, making it challenging for the Legislature to assess the adequacy of funding. We expect the Governor’s May Revision to include additional funding proposals related to Medi‑Cal county administration and H.R. 1 implementation, which may address some of the shortcomings we identify. If they do not, we recommend that the Legislature update statute to require a revised methodology by a certain date in the future.
Background
Medi‑Cal and CalFresh Are Among the Largest Health and Human Services (HHS) Programs. Medi‑Cal is California’s version of the federal Medicaid program. It provides health coverage to over 14 million low‑income people, or more than one‑third of all Californians. Total Medi‑Cal spending in 2024‑25 is estimated to have been $179 billion, including $37 billion from the General Fund. Of this amount, $2.4 billion ($629 million) was estimated to be for administration. CalFresh is California’s version of the federal Supplemental Nutrition Assistance Program. It provided federally funded food assistance to about 5.5 million low‑income Californians in 2024‑25 with total benefits of over $12.5 billion. The state also provides state‑funded food assistance benefits that are the same as CalFresh to about 60,000 additional low‑income legally present noncitizens who do not qualify for federal CalFresh benefits through the California Food Assistance Program (CFAP). CFAP benefits in 2024‑25 were $135 million. Hereafter, we consider CFAP as a state‑funded component of CalFresh. Administrative costs for CalFresh (and CFAP) in 2024‑25 are estimated to have been $2.5 billion ($925 million General Fund).
Counties Administer State HHS Programs
Counties Play Key Administrative Role for Medi‑Cal, CalFresh, and Other HHS Programs. At the state level, Medi‑Cal is overseen by the Department of Health Care Services (DHCS) and CalFresh is overseen by the Department of Social Services (DSS). Counties, however, are responsible for ground‑level program administration. In addition to Medi‑Cal and CalFresh, counties are also responsible for administration of other HHS programs, including California Work Opportunity and Responsibility to Kids (known as CalWORKs), which provides cash assistance and supportive services to low‑income families with children, and In‑Home Supportive Services (IHSS), which provides personal care and domestic services to elderly or disabled low‑income individuals to help them remain safely in their own homes and communities, among others.
County Administrative Responsibility Focused on Determining Eligibility. Eligibility determination involves assessing whether individuals applying for assistance in Medi‑Cal, CalFresh, or other HHS programs meet eligibility requirements such as those related to income, age, disability status, citizenship or immigration status, or family and household structure. Counties are also responsible for ensuring that only those who continue to meet eligibility requirements remain enrolled. This requires processing periodic renewals for each enrollee. Many individuals qualify for and enroll in more than one HHS program at a time. For example, an estimated 90 percent of CalFresh enrollees are also enrolled in Medi‑Cal. In recognition of this, eligibility determination and renewal processes are, to an extent, integrated across HHS programs. For example, there is a consolidated application form that can be used to apply to become enrolled in Medi‑Cal, CalFresh, and CalWORKs.
Federal, State, and County Governments Share Fiscal Responsibility for County Administration. Significant funding is allocated to support county administration of Medi‑Cal, CalFresh, and other major HHS programs. Figure 1 shows the distribution of fiscal responsibility across federal, state, and county governments for administration of key HHS programs. Today, among the major HHS programs, counties only have a share of cost for administration in CalFresh (although they may incur expenditures for costs beyond the state funds appropriated in the budget).
Figure 1
Funding Responsibility for Major HHS Program Administration
|
Estimated 2025‑26 Administration Funding |
Federal Share |
State Share |
County Sharea |
|
|
Medi‑Cal |
$2,378 |
Up to 75 percent |
Remaining costs |
No share |
|
CalFreshb |
2,641 |
50 percentc |
35 percent |
15 percent |
|
CalWORKs |
453 |
Variesd |
Remaining costs |
No sharee |
|
IHSSf |
959 |
50 percent |
50 percent |
No share |
|
aCounties may incur additional costs if expenditures exceed funding identified for administration in the annual state budget. bEstimated 2025‑26 funding includes $17.5 million for CFAP administration. CFAP administration is 100 percent state funded, with no federal or county shares. The shares shown in this row are for federal CalFresh administration only. cH.R. 1 reduces the federal share of cost beginning October 2026. dCalWORKS administration is partially funded with the state’s allocation from the federal TANF block grant. The state’s annual allocation is fixed and the portion of available grant funding spent on administration varies from year to year. eCounties are required to spend a minimum combined MOE amount on CalFresh and CalWORKs administration. In practice this requirement is met with CalFresh administration spending. fFor many years, counties had a 30 percent share of nonfederal costs for IHSS administration. Beginning in 2012‑13, counties have had an MOE requirement that requires the state to appropriate state funds for the nonfederal share of costs for IHSS administration. The federal share is 50 percent for individuals eligible for federal funding. Costs for certain individuals ineligible for federal funding are covered by state funds. |
||||
|
HHS = Health and Human Services; IHSS = In‑Home Supportive Services; CFAP = California Food Assistance Program; TANF = Temporary Assistance for Needy Families; and MOE = maintenance of effort. |
||||
State Spending on Administration Is Limited by Appropriation… The state budget limits the amount of state funds available for county administration of major HHS programs. This limit is proposed as part of the Governor’s budget. The Governor’s budget uses a variety of methodologies (each program has its own methodology) to estimate the amount of state funding that will be made available for county administration in each program. The amount of federal funding included in the Governor’s budget for each program is determined based on the proposed amount of state funds and in accordance with the sharing ratios and funding rules for each program. In the case of CalFresh, the Governor’s budget assumes that counties provide funding in an amount sufficient to access the full state appropriation and associated federal funds. In practice, however, total spending in CalFresh is driven by spending from county funds—to the extent that counties put up less county funding than the amount identified in the state budget, spending from state and federal funds will be reduced by a proportional amount, consistent with funding shares.
…But Counties May Spend Above Budget Amounts and Access Additional Federal Funds. On the other hand, counties may spend above the amounts assumed in the state budget. While state funds for county administration are limited by the state budget, counties in some cases may access additional federal funds beyond those that are matched by state dollars. They can do this by using county funds to draw down additional federal funds according to established sharing ratios (subject to federal approval), after state funds have been exhausted. This practice, sometimes referred to as county “overmatch,” is possible in CalFresh and IHSS and has been available in Medi‑Cal in the past, although not in recent years. For example, county spending on CalFresh administration is currently 15 percent of the total, until the state funds appropriation has been fully used. Thereafter, any additional county spending will be 50 percent of the total, with federal funds making up the remaining 50 percent. (Counties may spend above the amounts identified in the budget act for CalWORKs, but because federal funding for CalWORKs is fixed, there are no additional federal funds to match county expenditures.)
Counties Receive Realignment Revenues to Support Local Fiscal Responsibility. As described in the box below, some state sales tax and vehicle license fee revenue (hereafter “realignment revenues”) are deposited into a special fund dedicated to supporting responsibilities realigned from the state to counties. Some of this funding is used to support counties’ share of cost for CalFresh administration, among other county fiscal responsibilities such as providing basic health care for low‑income, uninsured individuals or covering a portion of benefit costs in IHSS.
What Is Realignment?
Realignments Typically Shift Responsibility, and Funding, From the State to the Counties. Realignment refers to changes in program responsibility, both administrative and fiscal, between the state and counties. Typically, realignments have shifted administrative responsibility and resources from the state to counties.
1991 Realignment Adjusted County Responsibility for Health and Human Services (HHS) Program Administration and Benefits… In 1991, the state enacted a major realignment package that, among other things, increased counties’ share of cost in some programs, while also reducing counties’ share of cost for administering major HHS programs, including CalFresh, the California Work Opportunity and Responsibility to Kids (CalWORKs) program, and In‑Home Supportive Services (IHSS). Counties were also given an increased share of state revenues to cover the net increase in costs.
…Subject to Later Changes. Over time, the state has modified the arrangement established through 1991 realignment. When CalWORKs was established in 1996 in response to federal welfare reform legislation, the state replaced a percentage share of cost for administration with a maintenance of effort (MOE) requirement that counties can meet with combined spending on CalFresh and CalWORKs administration. Beginning in 2012‑13, the state replaced a percentage share of cost for IHSS benefits and administration with an MOE requirement that grows over time. (In practice, the county MOE in IHSS is met with spending on benefits costs.) Today, CalFresh is the only remaining major HHS program for which counties have a percentage‑based share of cost through 1991 realignment.
H.R. 1 Notably Impacts Medi‑Cal and CalFresh Eligibility Administration
H.R. 1 was passed by Congress and signed by the President in July 2025. H.R. 1 introduces multiple significant changes to Medi‑Cal and CalFresh. Many of these changes, as described below, directly impact county administration in these programs. Changes will phase in over time, as shown in Figure 2.
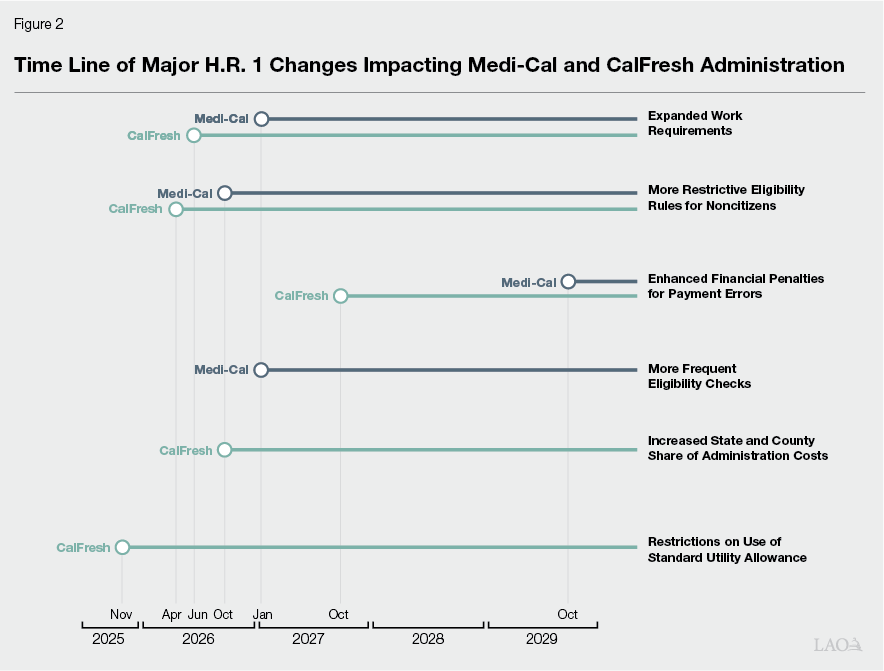
Expanded Work Requirements. H.R. 1 imposes a new work requirement in Medi‑Cal and expands an existing work requirement in CalFresh (although until recently the state has had a waiver from the CalFresh requirement for several years). While the details of how these changes affect each program vary, at a high level they require able‑bodied, working‑age adults without young dependent children to work or participate in other qualifying activities on a part‑time basis (approximately 20 hours per week). After accounting for potential exemptions, an estimated 3.5 million people are expected to become subject to the work requirement in Medi‑Cal beginning in January 2027. After accounting for exemptions, an estimated 845,000 people are expected to become subject to the expanded CalFresh work requirement beginning in June 2026. (An unknown, but likely significant, share of individuals subject to the CalFresh work requirement will also be subject to the Medi‑Cal work requirement.) Expanded work requirements create the need for counties to determine which enrollees are subject to the requirement and which are exempt, track the participation status of nonexempt individuals, and take action on their enrollment in accordance with that status.
More Restrictive Eligibility Rules for Noncitizens. H.R. 1 disqualifies certain noncitizen groups—including asylees, refugees, and others—from being eligible for federally funded, full‑scope Medi‑Cal and CalFresh assistance. This change will take effect in October 2026 in Medi‑Cal. The change in CalFresh was effective upon enactment of H.R. 1 but, due to the timing of federal guidance and the need to implement system changes and train county staff, is expected to be implemented in California in April 2026. An estimated 200,000 individuals are expected to lose Medi‑Cal and an estimated 72,000 are expected to lose CalFresh assistance due to this change.
Enhanced Financial Penalties for Payment Errors. As part of its oversight role, the federal government measures the extent to which payments for benefits and services in Medi‑Cal and CalFresh are provided only to eligible individuals and in amounts consistent with program rules. When payments are made in amounts that are inconsistent with program rules, it is considered to be a payment error. More details on payment error rates in Medi‑Cal and CalFresh are provided in a box below. Before H.R. 1, federal law imposed financial penalties on states when certain eligibility‑related payment errors in Medicaid exceeded a 3 percent threshold but also gave the federal oversight agency discretion to waive penalties when states made good‑faith efforts to reduce the error rate. Beginning October 2029, H.R. 1 expands the types of eligibility errors that are subject to penalties and restricts the good faith waiver. This increases the risk that California will be subject to penalties in Medi‑Cal in the future. Depending on the scope of such errors and forthcoming federal guidance influencing how the H.R. 1 penalties are implemented, they could potentially reach hundreds of millions or billions of dollars in a year.
Payment Error Rate Oversight in Medi‑Cal and CalFresh
Overview of Medicaid Payment Error Rate Measurement (PERM) Process. In Medicaid, the federal government undertakes triennial PERM reviews in each state that assess whether payments were made consistent with program requirements. The reviews look at errors in three main areas:
- Fee‑for‑Service (FFS). These errors relate to direct payments to health care providers. The most common reason for FFS errors is missing or inaccurate provider enrollment information.
- Managed Care. These errors relate to payments to managed care health plans. Among the three types of errors assessed in PERM, managed care errors make up a very small share.
- Eligibility. These errors relate to whether an individual was eligible to receive services. The most common reason for eligibility errors is that documentation was not collected or maintained to fully determine whether the individual was eligible at the time of the audit.
California’s most recent PERM review was in 2023. This review estimated an overall payment error rate in California of about 8 percent, of which about 70 percent was due to eligibility errors, with the rest attributable to FFS errors. Counties, in their role of administering Medi‑Cal eligibility determination, play a key role in eligibility errors but generally are not involved with FFS errors. For comparison, the average error rate for all states reviewed in 2023 was 6 percent.
Overview of Supplemental Nutrition Assistance Program (SNAP) Payment Error Rate (PER) Process. In SNAP, the federal government reviews a sample of cases each year to determine whether benefits provided were higher or lower than they should have been given the cases’ circumstances and from this calculates the error rate. The most common reasons for payment errors in California include unreported household income changes, inaccurate information on shelter costs, and delays in administrators acting on information that affects enrollees’ eligibility. California’s most recently measured PER was about 11 percent for federal fiscal year 2024. For comparison, the national average PER was also about 11 percent.
Payment Errors Do Not Necessarily Indicate Fraud. Fraud, or improperly obtaining or providing benefits through willful misrepresentation, is a type of improper payment. However, most instances of improper payment result from administrative errors or inadvertent omissions of needed information and are not fraud. These types of errors are driven, in part, by the significant complexity of Medi‑Cal and CalFresh for administrators and enrollees.
In CalFresh, H.R. 1 shifts a portion of federally funded SNAP benefit costs to states with an error rate of 6 percent or higher, beginning October 2027. As shown in Figure 3, states with higher error rates have a higher share of cost. If California’s payment error rate remains at its most recently measured level of 11 percent, the state would be liable for 15 percent of CalFresh benefits, resulting in about $2 billion in annual General Fund costs.
Figure 3
State Shares of CalFresh Benefit Costs for
Different Payment Error Rates
|
Payment Error Rate |
State Share of |
Approximate Annual |
|
Less than 6% |
— |
— |
|
From 6% to less than 8% |
5% |
$650 million |
|
From 8% to less than 10% |
10 |
1.3 billion |
|
10% or greater |
15 |
2 billion |
More Frequent Eligibility Checks in Medi‑Cal. Medi‑Cal enrollees are currently subject to annual eligibility redeterminations. Beginning January 2027, H.R. 1 requires that the state perform twice annual redeterminations for one group of Medi‑Cal enrollees—those who gained coverage through the Patient Protection and Affordable Care Act (ACA) expansion in 2014, commonly referred to as “childless adults.” (This is the same group to which H.R. 1 applies the new Medi‑Cal work requirement.) Doubling the frequency of redeterminations for this group, which includes an estimated 4.9 million individuals 2025‑26, increases county administration workload.
Increased State and County Share of CalFresh Administration Costs. Beginning October 2026, H.R. 1 reduces federal support for administrative costs from 50 percent to 25 percent. State law requires counties to cover 30 percent of the nonfederal share, meaning that the county share will increase to 22.5 percent and the state share will increase to 52.5 percent, as shown in Figure 4. This change is expected to result in ongoing annual costs of about $480 million for the state and $190 million for counties.
Figure 4
CalFresh Administration
Funding Responsibilities
|
Current |
Beginning |
|
|
Federal |
50.0% |
25.0% |
|
State |
35.0 |
52.5 |
|
Counties |
15.0 |
22.5 |
Restrictions on Use of Standard Utility Allowance (SUA) in CalFresh. The SUA is an option used in the CalFresh benefit determination that simplifies the benefit calculation and sometimes results in a household receiving a larger monthly CalFresh benefit than they would otherwise receive. One way to qualify to use the SUA is to receive a state‑funded utility assistance payment of at least $20.01 annually. Prior to H.R. 1, California provided such a utility payment to maximize household CalFresh benefits. Effective November 2025, H.R. 1 restricts the use of state‑funded utility assistance payments in this way to households with elderly or disabled members. This means that fewer households will be able to use the SUA, leading to reduced monthly benefits. 525,000 individuals are estimated to eventually have their CalFresh monthly benefits reduced by an estimated average of $39 from this change.
2025‑26 Spending Plan Provided Funding to Begin to Address H.R. 1 Implementation. Funding includes:
- $39.9 million ($20.1 million General Fund) for DSS to pursue data and technology changes and outreach to CalFresh beneficiaries to reduce the payment error rate and limit increased state costs for CalFresh benefits.
- Upon approval of the Department of Finance (DOF), up to $15 million General Fund for DSS to implement federal guidance on H.R. 1 implementation as it is released and up to $20 million to support county implementation of changes to the work requirement. These items have not yet been approved for release by DOF.
Governor’s Proposal
The Governor’s budget proposes $2.4 billion ($644 million General Fund) for Medi‑Cal county administration and $2.7 billion ($1.3 billion General Fund) for CalFresh administration in 2026‑27.
For Now, Maintains Current Level of Support for Medi‑Cal County Administration. The Governor’s proposed funding amount for Medi‑Cal administration is the same amount provided in 2024‑25 and 2025‑26. This is generally consistent with the state’s recent approach to funding Medi‑Cal administration since 2018‑19. In 2018‑19, the state began rolling forward the prior year’s budgeted amount for Medi‑Cal administration after applying a cost‑of‑living adjustment (COLA) based on projected inflation, with no adjustment for projected workload or enrollment. As a budget solution, the 2024‑25 spending plan suspended the COLA from 2024‑25 through 2027‑28. Since proposed administration funding is unchanged, the Governor’s budget makes no adjustment to account for the administrative impacts of implementing H.R. 1 requirements in Medi‑Cal in 2026‑27, including the work requirement and the more frequent redeterminations. The administration has indicated that it is working with counties to better understand H.R. 1 impacts on Medi‑Cal administration so that county administrative funding can be revisited at the May Revision.
Reflects Higher State and County Share of Cost for CalFresh Administration. To account for the lower federal share of cost for CalFresh administration under H.R. 1, the Governor’s budget reflects a $502 million reduction in federal funds, offset by a $359 million increase from the General Fund and $143 million increase from county funds.
Provides Some Additional Funding for Expanded CalFresh Work Requirement… As shown in Figure 5, the Governor’s budget provides additional funding—$8.4 million in 2025‑26 and $78.4 million in 2026‑27—for counties related to implementing the expanded CalFresh work requirement. This funding is related to automation; training county workers; and to account for county workers needing to engage with enrollees to assess whether they qualify for an exemption and, if not, whether they are meeting the requirement. Based on DSS assumptions about the hourly cost of eligibility workers, we estimate that funding provided in 2026‑27 to engage individuals subject to the work requirement is equivalent to a little over a one‑half hour per person initially subject to the requirement and about the same amount of time to engage again with those who are about to be discontinued due to not meeting the requirement. Under the administration’s budgeting methodology, we expect funding for these activities would likely decline after initial implementation as automation and training are completed and changes to enrollment are completed over 12 months.
Figure 5
Estimated H.R. 1 Impacts on CalFresh and CFAP Administration
(In Millions)
|
2025‑26 |
2026‑27 |
||||||||
|
Total |
Federal |
General Fund |
County |
Total |
Federal |
General Fund |
County |
||
|
ABAWD Work Requirement |
|||||||||
|
New administration and automation costsa |
$8.4 |
$4.2 |
$3.0 |
$1.2 |
$78.4 |
$24.3 |
$38.0 |
$16.1 |
|
|
Caseload impact |
— |
— |
— |
— |
‑78.6 |
‑24.4 |
‑38.1 |
‑16.1 |
|
|
Subtotals |
($8.4) |
($4.2) |
($3.0) |
($1.2) |
(‑$0.2) |
(‑$0.1) |
(‑$0.1) |
(—b) |
|
|
Noncitizen Eligibility Change |
— |
— |
— |
— |
‑$12.1 |
‑$2.5 |
‑$7.9 |
‑$1.7 |
|
|
SUAS Restriction |
‑$5.5 |
‑$2.7 |
‑$2.0 |
‑$0.8 |
‑$15.6 |
‑$4.8 |
‑$7.6 |
‑$3.2 |
|
|
Total Administrative Cost Changes |
$2.9 |
$1.5 |
$1.0 |
$0.4 |
‑$27.9 |
‑$7.4 |
‑$15.6 |
‑$4.9 |
|
|
Increased State and County Share of Costc |
— |
— |
— |
— |
— |
‑$502 |
$359 |
$143 |
|
|
aIncludes costs for training, automation, confirmation of work hours engagement, and processed discontinuances. Does not include funding for oral notice of work rules. bLess than $500,000. cEstimated H.R. 1 administrative impacts related to the ABAWD work requirement, noncitizen eligibility change, and SUAS restriction already reflect the increased state and county share of cost. Those impacts are also reflected in this line, resulting in minor overlap. |
|||||||||
|
CFAP = California Food Assistance Program; ABAWD = able‑bodied adult without dependents; and SUAS = State Utility Assistance Subsidy. |
|||||||||
…Offset by Reductions Accounting for Reduced Caseload. The state’s typical practice is to adjust CalFresh administrative funding by projected changes in enrollment, in recognition that higher or lower enrollment will result in higher or lower administrative costs. The Governor’s budget reduces funding for CalFresh administration to account for the various H.R. 1 policies that are anticipated to result in reduced CalFresh enrollment. Taken together, these assumed caseload savings more than offset additional funding provided to implement the expanded work requirement.
LAO Assessment
Supporting County Administration Is a Key Fiscal Priority
As front‑line administrators of Medi‑Cal and CalFresh, counties are critical to efforts to implement H.R. 1.
Minimizing Error Rates and Related Fiscal Penalties. Given the significant fiscal impacts involved, avoiding penalties for error rates is a high priority for the state, particularly in CalFresh. Potential penalties in Medi‑Cal are less certain and immediate but taking steps to limit payment errors in Medi‑Cal is also warranted. In carrying out their administrative responsibility, counties are required to follow state policy set by the Legislature and administratively by DHCS and DSS. DHCS and DSS policymaking activities underway now will accordingly shape counties’ H.R. 1 implementation. At the same time, individual county implementation will depend on strategies and resource allocation priorities of individual counties. To support successfully mitigating risks of payment error penalties, the Legislature will need to understand what changes to state and county processes will be required to address the largest contributors to error rates. DSS is currently engaged with counties in an in‑depth analysis of the root causes of the high CalFresh error rate. Preliminarily, income reporting appears to be a key focus.
Avoiding Disenrollment of Eligible Individuals. Research on the impacts of the SNAP work requirement indicate that it results in increased disenrollment, in part driven by otherwise eligible enrollees not complying with paperwork or tracking requirements (commonly referred to as “administrative burden”). Based on this, it is likely that some individuals who are in compliance with new requirements nevertheless will be disenrolled due to the additional administrative burden. Implementation of state work requirements in Medicaid programs nationwide has been limited to date, but we expect disenrollment due to administrative burden in Medi‑Cal as in CalFresh. In particular, processes that require manual verification or direct interaction with enrollees present risks that steps will be missed or information falls through the cracks. Automating verification processes and connecting with all available data sources to the extent possible is a key strategy to mitigating the risk that eligible individuals are disenrolled. In addition to automation, additional funding support for counties to allow more time to be spent with affected enrollees could also help mitigate incorrect disenrollments. To some extent, the benefit of additional funding will depend on how automation proceeds. As a result, it will be necessary to reevaluate any additional support provided over time as implementation proceeds.
Baseline Medi‑Cal Administration Budgeting Approach Has Shortcomings
Current Medi‑Cal Administration Budgeting Methodology Lacks Clear Link to Workload. While there is no clear indication that the current Medi‑Cal administration funding level is significantly out of alignment with costs, the current practice of holding funding flat year over year lacks an analytical basis that would allow the Legislature some assurance that funding is appropriately tied to workload. Without a methodology that links funding to workload, funding could become insufficient or exceed what is required for efficient operations without a clear way of assessing what adjustments are needed.
Legislatively Required Update Not Yet Completed. In 2013, the Legislature enacted statute requiring DHCS to develop a new methodology for budgeting Medi‑Cal administrative costs that would take into account significant changes in eligibility processes and much higher enrollment related to implementing the ACA in 2014. This new methodology was to be implemented no sooner than 2015‑16. Although efforts began to develop a revised methodology, none has been implemented to date. This is largely due to other competing policy priorities—for example ACA implementation and COVID‑19 response efforts. H.R. 1 will likely continue to strain the department’s ability to develop a revised methodology in the near term.
Other HHS Administration Budgeting Methodologies Include Useful Features. Despite the ongoing challenges the state and counties face in administering Medi‑Cal, it is important to consider steps toward developing a more rational budgeting methodology. The budgeting methodologies used for other major HHS programs are not perfect, but they do contain features that we believe would be valuable to consider applying to the Medi‑Cal context.
- Estimating Unit Costs Based on Actual Operations. The budgeting methodologies used for CalFresh and IHSS administration are both based on estimates of the average cost of performing typical eligibility tasks for each enrollee. In particular, DSS developed a revised CalFresh administration budgeting methodology, implemented starting in 2023‑24, that relies on estimates of unit costs for various mandated eligibility administration activities, based on a county survey. This approach creates a framework within which the Legislature can assess how best to adjust funding for county administration to respond to changing CalFresh program requirements, including H.R. 1 changes. As noted below, unit costs require updating from time to time to reflect changing operational conditions policy changes.
- Project Enrollment and Workload. Administrative budgeting methodologies used for CalFresh, IHSS, and CalWORKs all feature adjustments for changes in caseload. This feature is important because caseload generally is the most significant driver of changes in administrative workload. Other features of caseload adjustments in other programs may also be useful in Medi‑Cal. For example, the CalWORKs methodology puts some limits on the magnitude of year‑to‑year, caseload‑driven adjustments to administrative funding to minimize volatility that can be disruptive to counties. Another feature in the CalFresh administrative budgeting methodology relies on workload projections for different mandated activities (such as applications and recertifications). This allows for consideration of trends in eligibility activities that may not follow the overall caseload trend.
- Require That Assumptions Be Updated Periodically. One common challenge with HHS administration budgeting methodologies is that estimated unit costs and other assumptions can become outdated because of inflation or changes in processes or program requirements. In some cases, this can lead to counties making additional expenditures to cover costs above what can be covered with state funding approved in the budget act. To try to address this, the Legislature has taken steps to require that the administrative budgeting methodologies for both CalFresh and IHSS are reevaluated every three years, with a report to the Legislature on potential changes. (The most recent reevaluation of the IHSS methodology was for 2025‑26. We note however, that although the reevaluations were conducted, neither the Governor’s May Revision nor the 2025‑26 spending plan adopted any associated administrative changes identified in the DSS reassessment report.) COLAs can be another useful feature to mitigate the risk of budgeting methodologies falling out of alignment with costs.
H.R. 1 Puts Strain on State and County Budgets
State Faces Structural Deficit… Even before considering H.R. 1, our office and the administration estimate that the state faces significant structural budget deficits starting in 2027‑28. H.R. 1 adds to this structural budget problem. The impact on the state budget of higher administrative costs and a potential future benefit share in CalFresh is significant. The value of lost eligibility and benefits to Medi‑Cal and CalFresh enrollees is larger still. Addressing the structural budget problem will require difficult trade‑offs. Backfilling lost federal benefits under H.R. 1 would require billions of dollars in additional budget solutions.
…While Counties Face Multiple Cost Pressures. H.R. 1 also puts strain on county finances. As counties take on an estimated $190 million in new annual CalFresh administrative costs due to H.R. 1, state revenues provided to counties through 1991 realignment do not automatically adjust upward to account for these additional costs, beyond normal growth in revenues. This means that counties will need to reprioritize among other responsibilities. At the same time, counties face other cost pressures outside of HHS program administration and more related to direct services. H.R. 1 policies that result in disenrollment from Medi‑Cal will put pressure on county responsibility for indigent health. The Governor’s budget separately proposes to increase county responsibility for growth in IHSS benefit costs (in 2027‑28). Taken together, these cost pressures will make it challenging for counties to balance ongoing program operations and H.R. 1 implementation.
Recommendations
Direct Administration and Counties to Report on Drivers of Payment Error Rates and Plans to Manage Them. We recommend that the Legislature direct both the administration and counties to report at budget hearings on the major drivers of payment error rates and steps currently underway and future efforts to manage them in both Medi‑Cal and CalFresh. Some questions the Legislature may wish to consider asking the administration and counties to report on include:
- The impacts of changes to the Medicaid payment error rate in H.R. 1 are less certain and take effect later, relative to changes related to SNAP payment error rates. As a result, less information is available on the current status of the state’s compliance. What has been the state’s recent record of compliance with the Medicaid payment error rate requirements? What steps is DHCS taking to reduce the Medi‑Cal payment error rate in advance of H.R. 1 changes?
- What share of error rates is attributable to not having sufficient documentation versus incorrectly applying program rules to available information?
- What role do state policy decisions about eligibility processes play in affecting the complexity of operations and increasing or reducing the error rate in each program? Are there changes in state policy the state could consider that would reduce errors?
- What role do county policies and processes and the design and operation of automation and data systems play in determining the state’s error rates in each program? Do some counties have significantly higher or lower error rates than others and are there practices or other circumstances that contribute to this variation?
- How might recent and upcoming policy changes, including the recent discontinuation of eligibility flexibilities in Medi‑Cal in July 2025, upcoming implementation of work requirements in CalFresh and Medi‑Cal, and more frequent redeterminations in Medi‑Cal affect error rates in each program?
- To what extent are realignment funds used to support CalFresh administration today versus other county funds? How will increased county costs for CalFresh administration under H.R. 1 affect efforts to reduce payment error rates?
Weigh Trade‑Offs Between Additional Funding to Avoid Disenrollments Versus Other Priorities. Given the important role that counties play in implementing H.R. 1, the Legislature could consider providing additional funding for CalFresh administration, to allow counties to spend additional time working with enrollees to avoid disenrollment of eligible individuals. Similar additional funding could also be considered for Medi‑Cal after reviewing any changes the administration puts forward as part of the May Revision. In considering potential additional funding, the Legislature will need to weigh the benefit of any additional funding in terms of retained enrollment versus its other priorities and the need to address the state’s structural budget problem. If additional funding is provided, we recommend that the augmentation be temporary until the level of ongoing workload related to H.R. 1 is better understood following early implementation and can be reflected in ongoing funding methodologies. As part of its deliberations, the Legislature may wish to ask the administration to report on its plans for the $20 million made available to support county implementation of work requirements in CalFresh as part of the 2025‑26 spending plan.
Modify Statute to Establish a Deadline for a Revised Medi‑Cal County Administration Budgeting Methodology. We expect the Governor’s May Revision to include additional funding proposals related to Medi‑Cal county administration and H.R. 1 implementation. These proposals may address some of the shortcomings we identify in the underlying budgeting methodology. If these shortcomings are not addressed in a May Revision proposal, we recommend that the Legislature update statute to require a revised methodology by a certain date in the future. The new date should take into account that it may take time to fully understand and incorporate the impacts of HR 1 into an administrative funding methodology. Additionally, in taking this task on, the administration will be adding to the many competing priorities that are underway. This means that temporary funding may need to be in place until ongoing methodologies can be established.